Nervous Tissue: Understanding Pain Transmission and Its Role in Physical Therapy
Learn how nervous tissue transmits pain signals, how the nervous system adapts to injury, and how physical therapy uses neuroscience to reduce pain and restore function.
Pain is one of the most common reasons people seek physical therapy. Whether it originates from a fresh injury, a chronic condition, post-surgical recovery, or a neurological disorder, pain is always a product of the nervous system. And because the nervous system is both the source of pain and the target of many physical therapy interventions, understanding nervous tissue is essential for anyone involved in rehabilitation.
This article explores the structure and function of nervous tissue, the biology of pain transmission, and how physical therapy works with — rather than against — the nervous system to reduce pain and restore movement.
What Is Nervous Tissue?
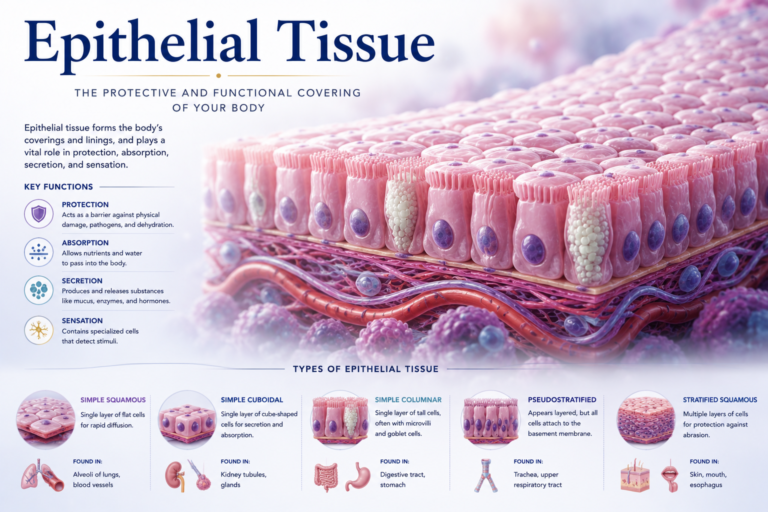
Nervous tissue is one of the four primary tissue types in the human body. It is found throughout the central nervous system (brain and spinal cord) and the peripheral nervous system (nerves outside the brain and spinal cord). It is composed of two main cell types: neurons and glial cells.
Neurons are the electrically excitable cells that transmit information in the form of electrical impulses (action potentials). Each neuron has three main components:
- Dendrites: Branch-like projections that receive signals from other neurons or from sensory receptors.
- Cell body (soma): Contains the nucleus and carries out the cell’s metabolic functions.
- Axon: A single, long projection that transmits the electrical signal away from the cell body toward the next neuron or target tissue (such as a muscle).
Glial cells (or glia) support, protect, and maintain neurons. They far outnumber neurons in the nervous system. Key types include Schwann cells (which form the myelin sheath around peripheral nerve axons) and astrocytes, oligodendrocytes, and microglia in the central nervous system.
Myelin is a fatty insulating layer that wraps around axons, dramatically increasing the speed of signal transmission. Demyelinating conditions — such as multiple sclerosis — severely disrupt nervous system function and are increasingly addressed through specialized neurological physical therapy.
How the Nervous System Transmits Pain
Pain is not a simple direct signal from injured tissue to the brain. It is a complex, multi-stage process involving specialized sensory neurons, spinal cord processing, and brain interpretation. Understanding this process helps explain both why pain sometimes persists long after an injury has healed and why physical therapy can be so effective at reducing it.
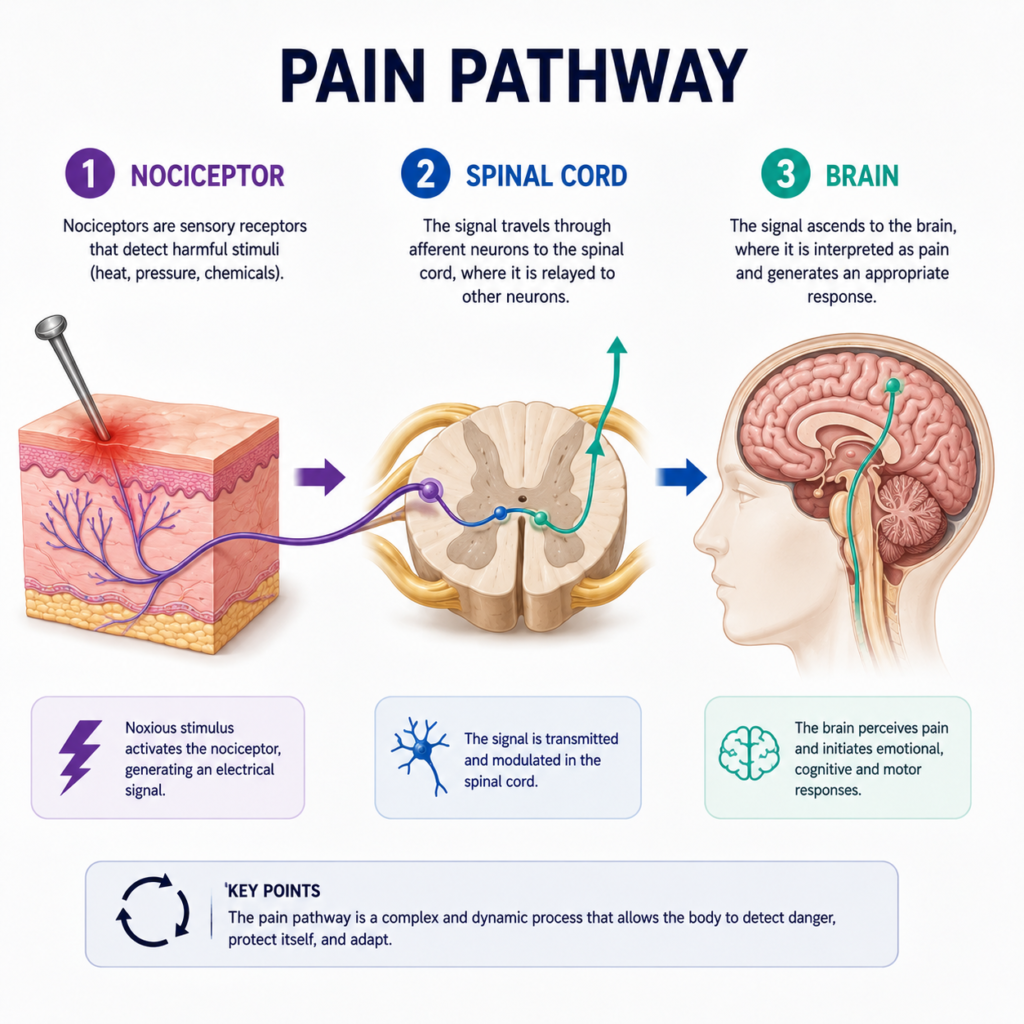
Step 1 — Nociception: Pain begins when nociceptors — free nerve endings in tissues — are activated by potentially harmful stimuli: mechanical pressure, extreme temperatures, or chemicals released by damaged cells (such as prostaglandins, bradykinin, and substance P). These signals travel along two types of afferent (sensory) nerve fibers:
- A-delta fibers: Myelinated, fast-conducting fibers that transmit sharp, acute pain (the initial “ouch” of an injury).
- C fibers: Unmyelinated, slow-conducting fibers that carry dull, throbbing, or burning pain — the longer-lasting component.
Step 2 — Spinal processing: The pain signal reaches the dorsal horn of the spinal cord, where it synapses with interneurons. Here, the signal can be modulated — amplified or dampened — before it ascends to the brain. Gate control theory (proposed by Melzack and Wall) describes how non-painful sensory input (touch, vibration, movement) can “close the gate” on pain signals at the spinal cord level. This is one mechanism through which physical therapy interventions like massage and joint mobilization reduce pain.
Step 3 — Brain processing: The signal travels via the spinothalamic tract to the thalamus and then to multiple brain areas, including the somatosensory cortex (where the location and intensity of pain are processed), the limbic system (emotional response), and the prefrontal cortex (cognitive appraisal). Pain is ultimately an experience created by the brain — which is why psychological factors like anxiety, fear of movement, and catastrophizing strongly influence pain perception.
Peripheral Sensitization and Central Sensitization
After an injury, the nervous system can become sensitized — more responsive to input than normal. This sensitization is one of the key mechanisms underlying chronic pain.
Peripheral sensitization occurs at the site of injury. Inflammatory chemicals lower the threshold of nociceptors, making them respond to stimuli that would not normally be painful (allodynia) or respond more strongly to painful stimuli (hyperalgesia). This is why a sunburned shoulder is exquisitely sensitive to gentle touch.
Central sensitization occurs in the spinal cord and brain. When pain signals are sustained, they can trigger changes in spinal cord neurons that amplify all sensory input from the affected area. This leads to widespread, persistent pain that outlasts the original tissue injury — a major feature of conditions like fibromyalgia, complex regional pain syndrome (CRPS), and chronic low back pain.
Physical therapy targets both types of sensitization. Manual therapy and exercise reduce peripheral sensitization by decreasing local inflammation and promoting tissue healing. Education, gradual exposure to movement, and graded exercise target central sensitization by retraining the nervous system’s response to input.
Neuroplasticity: The Brain’s Ability to Change
One of the most important discoveries in modern neuroscience is that the adult nervous system is not fixed. It has remarkable plasticity — the ability to reorganize its structure and function in response to experience, learning, injury, and rehabilitation.
After an injury, neuroplasticity can work against the patient: the brain may develop maladaptive representations of the affected body part, increasing pain sensitivity and disrupting motor control. This is seen in conditions like phantom limb pain and some cases of chronic low back pain.
But neuroplasticity also enables recovery. Repetitive, task-specific exercise creates new neural connections, strengthens motor patterns, and can literally reorganize brain maps of the body. This is the foundation of neurological rehabilitation — after stroke, spinal cord injury, or nerve damage, repeated practice of purposeful movement gradually restores function by retraining the nervous system.
Physical therapists working with chronic pain patients increasingly use pain neuroscience education — teaching patients to understand their nervous system and the nature of pain — as part of treatment. Research consistently shows that understanding pain reduces fear of movement and improves rehabilitation outcomes.
Nerve Injuries and Physical Therapy
Peripheral nerve injuries are classified by severity:
- Neuropraxia: Temporary loss of function due to compression or mild stretching, without structural damage. Full recovery is expected.
- Axonotmesis: Axon damage with the outer connective tissue sheath intact. Regeneration is possible but slow (nerves regenerate at approximately 1mm per day).
- Neurotmesis: Complete nerve division. Surgical repair may be needed; recovery is incomplete.
Physical therapy for nerve injuries includes nerve gliding exercises (to restore mobility of the nerve within its surrounding tissues), sensory re-education (to retrain the brain’s interpretation of sensory input), progressive strengthening of affected muscles, and functional retraining.
Conclusion
Nervous tissue is not just the carrier of pain signals — it is a dynamic, adaptable system that can be trained, retrained, and optimized through physical therapy. From gate control theory to neuroplasticity, the neuroscience of pain and recovery provides compelling evidence that physical therapy works through real biological mechanisms — not just by making patients “feel better” through distraction.
For patients with acute injuries, the nervous system is the mediator of pain that guides their rehabilitation. For patients with chronic conditions, it is the central target of treatment. In all cases, understanding how nervous tissue works empowers patients to engage more confidently and effectively with their physical therapy programs.
References
- Ross, M.H., & Pawlina, W. (2020). Histology: A Text and Atlas (8th ed.). Wolters Kluwer.
- Mescher, A.L. (2021). Junqueira’s Basic Histology: Text and Atlas (16th ed.). McGraw-Hill.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.