Muscle Tissue: How Muscles Contract, Why They Get Injured, and How They Heal
Learn how skeletal muscle tissue is structured, how it contracts, why it gets injured, and how physical therapy supports muscle repair and recovery.
Muscle tissue is one of the most dynamic and adaptable tissues in the human body. It powers every voluntary movement — from the smallest flicker of a finger to the explosive force of a sprint. But muscle is also one of the most commonly injured tissues, accounting for a large proportion of cases seen in physical therapy practice.
To understand muscle injuries and their treatment, we need to understand what muscle tissue is, how it contracts, why it fails under certain conditions, and how it repairs itself. This knowledge sits at the core of effective physical therapy for musculoskeletal conditions.
Structure of Skeletal Muscle
The human body contains over 600 skeletal muscles. Each muscle is composed of many individual muscle fibers (muscle cells, or myocytes). A single muscle fiber can be several centimeters long and contains hundreds of nuclei — an unusual feature that reflects the unique developmental origin of muscle cells, which form by the fusion of many precursor cells.
Each muscle fiber is packed with myofibrils — thin, cylindrical structures that run the length of the cell and are the contractile units of muscle. Myofibrils are composed of repeating units called sarcomeres, which are the basic functional units of muscle contraction.
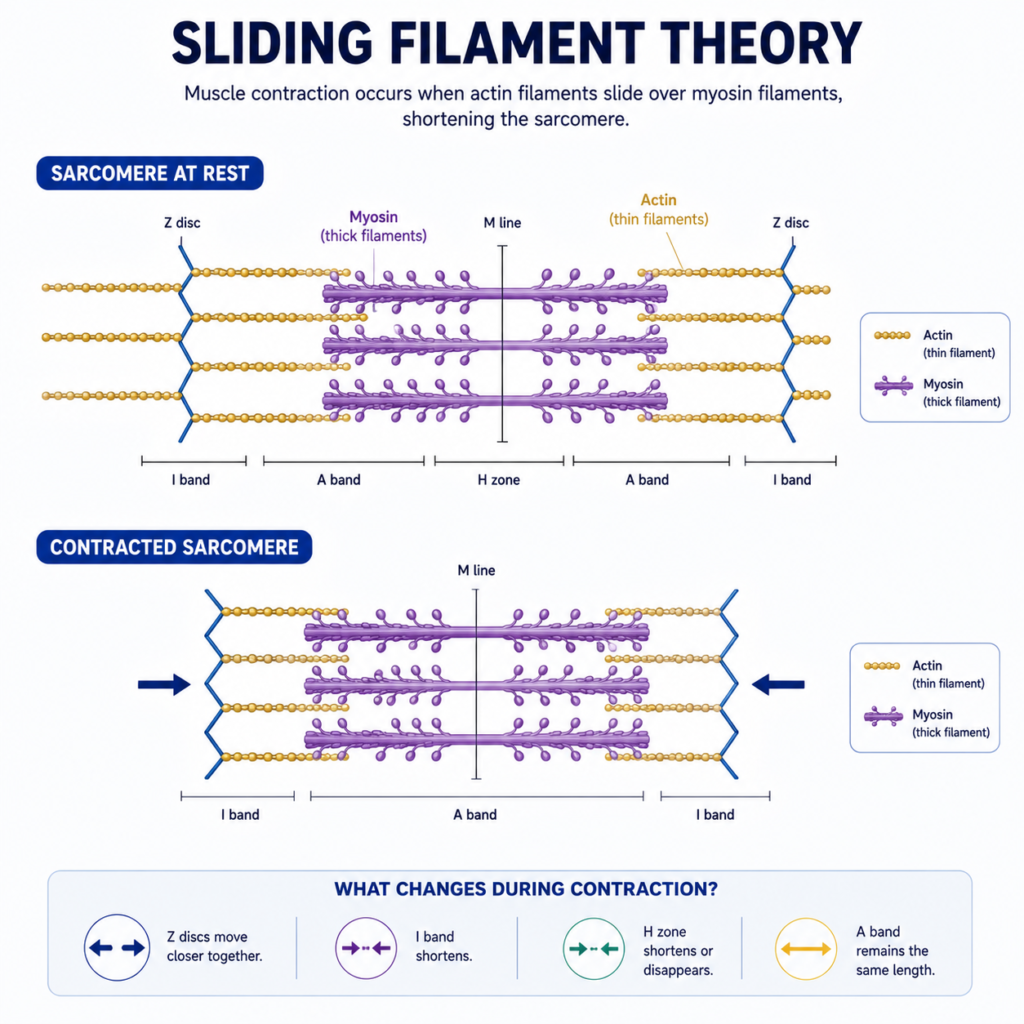
The sarcomere contains two main types of protein filaments:
- Actin (thin filaments): Two strands of actin wound around each other, anchored at the Z-discs at each end of the sarcomere.
- Myosin (thick filaments): Bipolar filaments with globular “heads” that project outward and are capable of binding to actin.
The regular arrangement of these filaments gives skeletal muscle its characteristic striped (striated) appearance under the microscope. The ratio and density of actin and myosin filaments determine the force-generating capacity of the muscle fiber.
The Sliding Filament Theory: How Muscles Contract
Muscle contraction is explained by the sliding filament theory. During contraction, the actin and myosin filaments do not shorten — instead, they slide past each other, reducing the length of the sarcomere and, collectively, the muscle fiber.
This sliding is powered by myosin heads acting as molecular motors. The process works as follows:
- A nerve impulse arrives at the neuromuscular junction and triggers the release of acetylcholine (a neurotransmitter).
- Acetylcholine binds to receptors on the muscle cell membrane, generating an electrical signal (action potential) that travels along the membrane and into the cell via a system of tubes called T-tubules.
- The action potential reaches the sarcoplasmic reticulum (the muscle cell’s smooth ER), triggering the release of calcium ions into the cytoplasm.
- Calcium binds to troponin, a regulatory protein on the actin filament. This causes a conformational change that exposes the binding sites on actin.
- Myosin heads bind to actin, forming cross-bridges. Using energy from ATP, the myosin head swings, pulling the actin filament inward. This is the “power stroke.”
- The myosin head releases actin, returns to its starting position, and the cycle repeats as long as calcium and ATP are available.
When the nerve signal stops, calcium is pumped back into the sarcoplasmic reticulum, the binding sites on actin are re-covered, and the muscle relaxes.
This entire process depends on a continuous supply of ATP — which is why energy metabolism is so critical to muscle function.
Muscle Fiber Types and Physical Therapy Implications
Not all muscle fibers are the same. They are broadly classified into two main types:
Type I (slow-twitch) fibers contract slowly, generate moderate force, and are highly resistant to fatigue. They are packed with mitochondria and rely primarily on aerobic metabolism. Type I fibers are dominant in postural muscles and are recruited first during low-intensity, sustained activities.
Type II (fast-twitch) fibers contract quickly and generate large amounts of force, but fatigue more rapidly. They rely more on anaerobic metabolism. Type IIx fibers are the fastest and most powerful but exhaust most quickly; Type IIa fibers are intermediate.
Physical therapy programs are designed with these fiber types in mind. Endurance training (low load, high repetitions, sustained exercise) preferentially trains Type I fibers and improves aerobic capacity. Strength training (high load, low repetitions) recruits Type II fibers and drives hypertrophy.
After injury or prolonged immobilization, muscles often lose Type II fiber properties disproportionately — a phenomenon called muscle atrophy. Rehabilitation protocols that include progressive resistance exercise are specifically designed to restore the strength and power capacity of these fast-twitch fibers.
Common Muscle Injuries in Physical Therapy
Muscle injuries range from mild delayed onset muscle soreness to severe complete ruptures. The most common presentations in physical therapy include:
Muscle strains (tears) occur when muscle fibers are stretched beyond their capacity or contract forcefully while being lengthened. They are graded I (minor), II (partial tear), and III (complete rupture). The hamstring, calf (gastrocnemius), and quadriceps are commonly strained in sports. Physical therapy rehabilitation progresses through pain-free range of motion, progressive strengthening, and sport-specific movement training.
Delayed onset muscle soreness (DOMS) is the familiar soreness that peaks 24-72 hours after unaccustomed exercise, particularly eccentric exercise (movements where the muscle lengthens under load, such as downhill running). DOMS results from microscopic muscle fiber damage and the subsequent inflammatory response. It is not harmful and actually represents the stimulus for muscle adaptation. Light activity, gentle stretching, and progressive loading help manage DOMS and speed recovery.
Muscle contusions result from direct blows to the muscle (such as in contact sports) and involve bleeding into the muscle tissue. Physical therapy focuses on controlling the initial hematoma, restoring range of motion, and progressively rebuilding strength.
Compartment syndrome occurs when pressure within a muscle compartment rises to dangerous levels — a medical emergency requiring immediate intervention.
Muscle Regeneration: The Role of Satellite Cells
Skeletal muscle has a significant capacity for regeneration, primarily due to a population of stem cells called satellite cells. These cells lie dormant along the surface of muscle fibers until activated by injury or exercise.
When a muscle fiber is damaged, satellite cells activate, divide, and either fuse with the damaged fiber (restoring its nuclei and regenerative capacity) or generate entirely new muscle fibers. This remarkable process allows muscles to recover from injuries that would be permanent in tissues with less regenerative capacity.
Physical therapy interventions support muscle regeneration by:
- Providing controlled mechanical loading that activates satellite cells.
- Promoting blood flow and nutrient delivery to the healing muscle.
- Preventing excessive scar tissue formation through early, gentle movement.
- Stimulating growth factor release through exercise.
Practical Takeaways for Physical Therapy Patients
Understanding muscle tissue biology has direct implications for rehabilitation:
Progressive overload is essential. Muscles only grow and strengthen when they are challenged beyond their current capacity. Physical therapy programs that are too easy fail to provide the stimulus needed for tissue adaptation.
Eccentric exercise is especially important. Research consistently shows that eccentric exercises (such as Nordic hamstring curls, heel drops for Achilles tendinopathy, and wall squats) are among the most effective ways to stimulate connective tissue and muscle adaptation.
Full recovery takes time. Muscle tissue repair unfolds over weeks to months. Pain resolution does not mean the muscle has fully healed — returning to full load too quickly risks re-injury.
Nutrition matters. Adequate protein intake (especially leucine-rich proteins), along with vitamins D and C, supports muscle protein synthesis during recovery.
Conclusion
Muscle tissue is a masterpiece of biological engineering — capable of generating force, adapting to demands, and repairing itself from injury. The sarcomere is the fundamental unit of contraction; the satellite cell is the guardian of regeneration; and the physical therapist is the guide who provides the optimal conditions for this biology to do its work.
Every therapeutic exercise, every manual technique, every session of rehabilitation provides signals that cascade through muscle tissue at the cellular level. Understanding this biology allows patients and practitioners alike to make more informed decisions about how to approach recovery — and why some paths lead to lasting results while others fall short.
References
- Ross, M.H., & Pawlina, W. (2020). Histology: A Text and Atlas (8th ed.). Wolters Kluwer.
- Mescher, A.L. (2021). Junqueira’s Basic Histology: Text and Atlas (16th ed.). McGraw-Hill.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.