Lipids and Fats: Beyond Energy Storage and Their Role in Physiotherapy
Explore the many roles of lipids in the human body — from cell membrane structure to inflammation regulation — and how fat metabolism supports physical therapy recovery.
For decades, fat had a bad reputation. Dietary fat was blamed for obesity, heart disease, and numerous other health problems. But as our understanding of biochemistry has deepened, we have come to appreciate that lipids — the broad category that includes fats, oils, phospholipids, and steroids — are far more than just stored energy. They are essential structural components of every cell, key regulators of inflammation, precursors to critical hormones, and important partners in recovery.
For physical therapy patients, understanding lipid biochemistry helps explain why a balanced diet rich in the right types of fats supports healing, why inflammation follows predictable patterns, and how fat metabolism contributes to the energy that powers rehabilitation exercises.
What Are Lipids?
Lipids are a diverse group of molecules defined by one shared property: they are hydrophobic (water-repelling). This property arises from their predominantly hydrocarbon structure, which lacks the polar groups that would allow interaction with water.
The main categories of lipids relevant to human physiology are:
Triglycerides (triacylglycerols): The most abundant lipid in the body and the primary form of dietary fat. A triglyceride consists of a glycerol backbone with three fatty acid chains attached. Triglycerides are stored in adipose tissue (body fat) and serve as the body’s largest energy reserve.
Phospholipids: The primary structural component of all cell membranes. A phospholipid has a polar (water-attracting) head and two nonpolar (water-repelling) fatty acid tails. This amphipathic structure causes phospholipids to spontaneously form bilayers in aqueous environments — the foundation of the cell membrane.
Sterols (including cholesterol): Cholesterol is an essential structural component of animal cell membranes and the precursor to steroid hormones (including cortisol, testosterone, estrogen, and progesterone), bile acids, and vitamin D.
Fatty acids: The basic building blocks of triglycerides and phospholipids. They consist of a carboxyl group attached to a hydrocarbon chain. Their length and degree of saturation determine their physical properties and metabolic effects.
Fatty Acids: Saturated, Monounsaturated, and Polyunsaturated
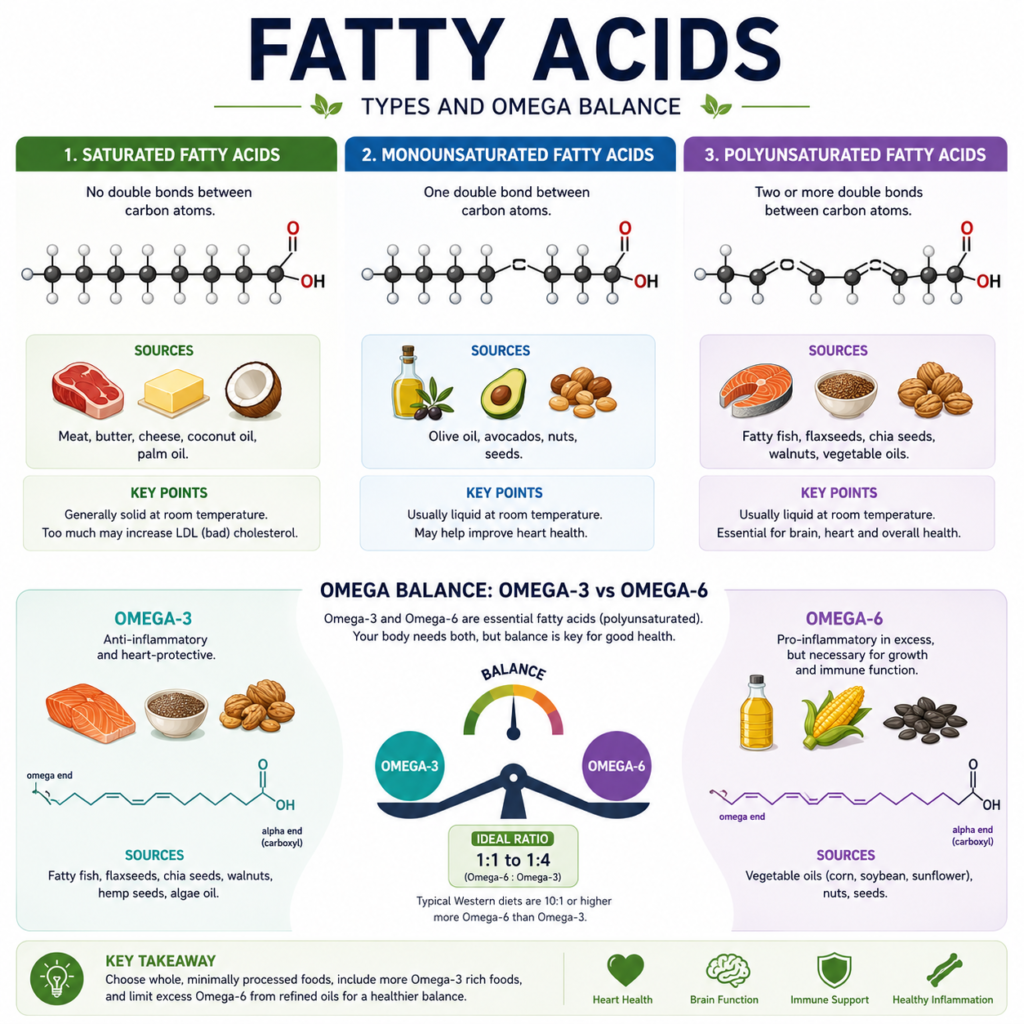
Fatty acids are classified by their degree of saturation — the number of double bonds between carbon atoms:
Saturated fatty acids have no double bonds; all carbons are saturated with hydrogen atoms. They tend to be solid at room temperature (like butter and coconut oil). The body can synthesize saturated fatty acids, so they are not essential in the diet.
Monounsaturated fatty acids (MUFAs) have one double bond. Oleic acid — the main fatty acid in olive oil — is the best-known MUFA. MUFAs are associated with cardiovascular benefits and reduced inflammation.
Polyunsaturated fatty acids (PUFAs) have two or more double bonds. The most critical PUFAs for human health are the essential fatty acids, which the body cannot synthesize:
- Omega-6 fatty acids (primarily linoleic acid, found in vegetable oils) — the precursors to pro-inflammatory eicosanoids.
- Omega-3 fatty acids (primarily EPA and DHA, found in fatty fish; and ALA, found in flaxseeds and walnuts) — the precursors to anti-inflammatory eicosanoids.
The balance between omega-6 and omega-3 intake has profound implications for inflammation — and therefore for tissue healing and physical therapy outcomes.
Lipids and Inflammation: The Omega-3/Omega-6 Balance
One of the most clinically relevant aspects of lipid biochemistry for physical therapy is the role of fatty acids in regulating inflammation. The body uses polyunsaturated fatty acids as precursors to a family of powerful signaling molecules called eicosanoids — which include prostaglandins, leukotrienes, and thromboxanes.
Omega-6 fatty acids are precursors to pro-inflammatory eicosanoids (like prostaglandin E2). Omega-3 fatty acids compete with omega-6s for the same enzymes and produce anti-inflammatory eicosanoids (like resolvin E1 and protectin D1).
In the typical modern diet, the omega-6 to omega-3 ratio is approximately 15-20:1 — far higher than the 4:1 or lower ratio that appears optimal for health. This imbalance promotes a pro-inflammatory state that can contribute to chronic pain, slower tissue healing, and increased risk of inflammatory conditions.
Physical therapy patients can benefit from increasing omega-3 intake through fatty fish (salmon, mackerel, sardines), fish oil supplements, flaxseeds, chia seeds, and walnuts. Several studies suggest that omega-3 supplementation reduces muscle soreness after exercise, accelerates recovery from muscle damage, and may help manage inflammation in conditions like rheumatoid arthritis and tendinopathy.
Cholesterol: Essential, Not Just Harmful
Despite its negative reputation, cholesterol is an absolutely essential molecule. The body produces approximately 1000mg of cholesterol per day — a testament to how critical it is for normal function.
Cholesterol maintains the fluidity and structural integrity of cell membranes. Without adequate membrane cholesterol, cells cannot function properly. Cholesterol is the precursor to:
- Steroid hormones: Cortisol (the stress hormone that also regulates inflammation), testosterone and estrogen (which influence muscle mass, bone density, and recovery), aldosterone (which regulates blood pressure and fluid balance), and progesterone (important in reproductive physiology).
- Vitamin D: Synthesized from cholesterol in the skin upon UV exposure. Vitamin D is essential for calcium absorption, bone health, and immune function — all directly relevant to physical therapy patients.
- Bile acids: Produced in the liver and necessary for the digestion and absorption of dietary fats.
For physical therapy patients with musculoskeletal conditions, adequate vitamin D and steroid hormone levels significantly influence recovery. Low vitamin D is associated with muscle weakness, increased fracture risk, and impaired immune function.
Fat as an Energy Source in Physical Therapy Exercise
While carbohydrates are the preferred fuel during high-intensity exercise, fats become increasingly important as an energy source during lower-intensity, longer-duration activity. This is the metabolic zone most commonly targeted during early rehabilitation — gentle walking, cycling, aquatic therapy, and low-impact aerobic exercise.
Triglycerides in adipose tissue are broken down through a process called lipolysis, releasing fatty acids into the blood. These fatty acids are taken up by muscle cells and transported into the mitochondria, where they undergo beta-oxidation — a series of reactions that progressively cleave the fatty acid chain into two-carbon units, producing acetyl-CoA, which feeds into the Krebs cycle to generate ATP.
Fat provides more than twice as much energy per gram as carbohydrates (9 kcal/g vs. 4 kcal/g), making it an ideal long-term fuel for sustained low-intensity exercise. The body’s fat stores are vast — even a lean person carries enough stored fat to fuel several hours of moderate exercise.
Regular aerobic exercise — including the cardiovascular components of physical therapy programs — increases the body’s ability to oxidize fat. This metabolic adaptation (increased fat burning capacity) is one of the reasons aerobic fitness improves endurance and reduces reliance on glycogen during exercise.
Lipids in Joint Health: Synovial Fluid
Synovial fluid — the fluid that lubricates synovial joints — contains lipids that contribute to its lubricating properties. Phospholipid bilayers on the cartilage surface and in synovial fluid create an almost frictionless bearing surface. Disruption of this lipid layer through inflammation or degeneration contributes to the increased friction and pain seen in arthritic joints.
Some research suggests that joint supplementation with omega-3 fatty acids may help maintain the quality of synovial fluid and reduce joint inflammation in conditions like osteoarthritis. While the evidence is still evolving, this represents an interesting interface between lipid biochemistry and joint health management.
Conclusion
Lipids are indispensable to human health — providing structural integrity to every cell membrane, regulating the inflammatory response, serving as precursors to essential hormones and vitamins, and fueling sustained physical activity. In the context of physical therapy, paying attention to dietary fat quality — particularly optimizing the omega-3/omega-6 balance — can meaningfully support the healing process and improve outcomes.
Understanding that “fat” is not a single entity but a diverse family of molecules with profoundly different biological effects empowers physical therapy patients to make dietary choices that support rather than hinder their recovery.
References
- Nelson, D.L., & Cox, M.M. (2021). Lehninger Principles of Biochemistry (8th ed.). W.H. Freeman.
- Berg, J.M., Tymoczko, J.L., Gatto, G.J., & Stryer, L. (2019). Biochemistry (9th ed.). W.H. Freeman.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.