Inflammation: Friend or Foe in Physical Therapy Recovery?
Understand the biology of inflammation — why it is necessary for healing, when it becomes problematic, and how physical therapy manages inflammation for optimal recovery.
Few biological processes are as misunderstood as inflammation. Popular culture treats it as an enemy — something to be suppressed with ice packs, anti-inflammatory drugs, and rest at all costs. Yet inflammation is, in its acute form, an essential and purposeful biological response without which tissue healing simply cannot occur. The challenge is not to eliminate inflammation, but to understand it well enough to support the beneficial phases while preventing the harmful ones.
This distinction is central to modern physical therapy. Therapeutic decisions about when to apply ice or heat, when to encourage movement versus rest, and how to time the introduction of exercise all depend on a nuanced understanding of the inflammatory process. This article explains the biology of inflammation, distinguishes between its helpful and harmful forms, and describes how physical therapy approaches the management of inflammation to optimize recovery.
What Is Inflammation?
Inflammation is the body’s immediate response to tissue damage or infection. The word comes from the Latin inflammare — “to set on fire” — reflecting the heat that is one of its cardinal signs. The classic signs of acute inflammation, first described by the Roman physician Celsus, are:
- Rubor (redness) — from increased blood flow
- Calor (heat) — from increased metabolism and blood flow
- Tumor (swelling) — from fluid accumulation in tissue
- Dolor (pain) — from chemical mediator activation of nociceptors
- Functio laesa (loss of function) — from pain and swelling
A fifth sign was added by Virchow in the 19th century: functio laesa (loss of function). All five signs reflect the same underlying biological events: vasodilation, increased vascular permeability, fluid exudation into tissue, and immune cell infiltration.
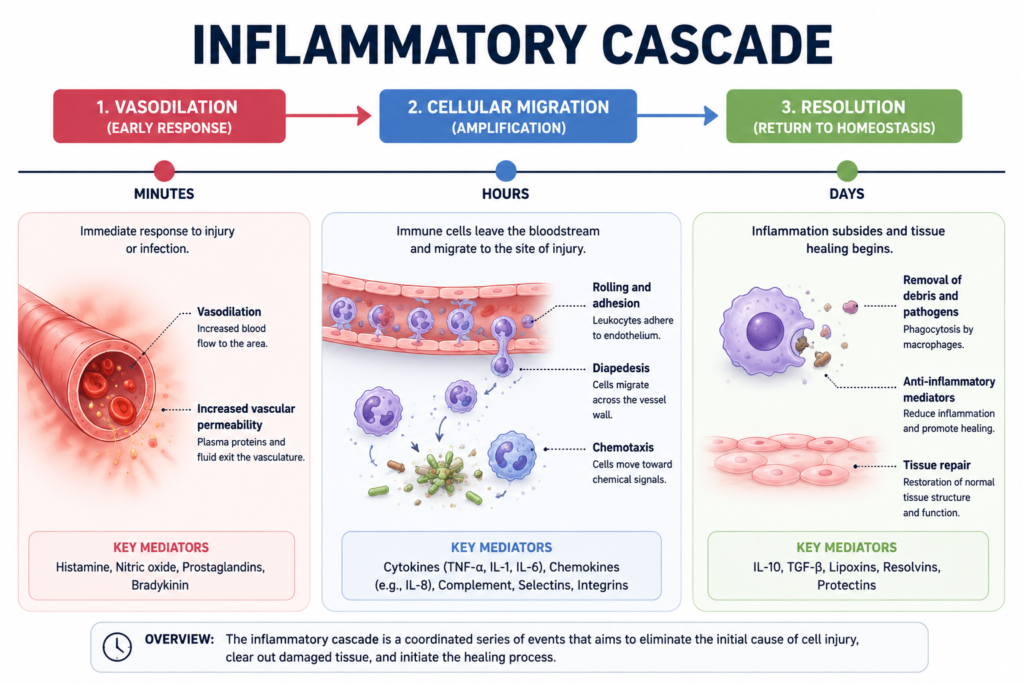
The Inflammatory Cascade: A Step-by-Step Process
When tissue is damaged — whether by physical injury, surgery, overuse, or infection — a precisely orchestrated cascade of events is set in motion:
Step 1 — Damage recognition: Injured cells release damage signals (DAMPs), and pathogens release pathogen signals (PAMPs). These are detected by pattern recognition receptors on resident immune cells, particularly mast cells and macrophages.
Step 2 — Vasoactive mediator release: Mast cells release histamine and serotonin, causing immediate vasodilation and increased vascular permeability. Bradykinin (generated from plasma proteins) amplifies these effects. This is why an injury becomes red and warm within seconds to minutes.
Step 3 — Prostaglandin production: Injured cells (and activated immune cells) produce arachidonic acid from their membrane phospholipids and convert it to prostaglandins via the COX (cyclooxygenase) enzymes. Prostaglandins are key inflammatory mediators that:
- Lower the pain threshold of nociceptors (sensitizing them — explaining why injured tissue is extra sensitive).
- Promote fever.
- Amplify vasodilation.
This is why NSAIDs (which block COX enzymes) are effective pain relievers and anti-inflammatories.
Step 4 — Neutrophil infiltration: Cytokines released by mast cells and macrophages attract neutrophils from the bloodstream. Neutrophils squeeze through the vessel wall (diapedesis) and migrate to the injury site along chemical gradients (chemotaxis). They phagocytose bacteria and debris and release enzymes and reactive oxygen species that destroy pathogens.
Step 5 — Macrophage predominance: As neutrophils complete their work (and undergo apoptosis), macrophages become the dominant cell. Early macrophages (M1 phenotype) continue the clean-up and produce pro-inflammatory cytokines (TNF-α, IL-1β, IL-6). Later, macrophages shift to M2 phenotype — producing anti-inflammatory signals and growth factors that initiate tissue repair.
Step 6 — Resolution: Specialized pro-resolving mediators (SPMs) derived from omega-3 fatty acids signal the end of the inflammatory response. Immune cells leave the tissue, and the repair process begins.
This entire acute inflammatory response normally completes within 3-7 days for most musculoskeletal injuries.
Why Inflammation Is Necessary
Suppressing inflammation entirely — particularly in the early stages — impairs healing. Here is why each component of the inflammatory response is necessary:
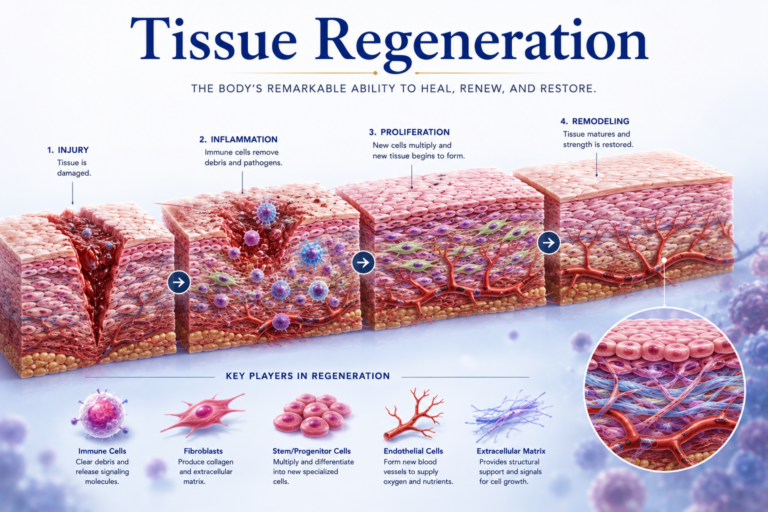
Neutrophils must clear debris. Before new tissue can be laid down, the damaged material must be removed. Blocking neutrophil function or activity prematurely leaves a mess of cellular debris that prevents proper repair.
Macrophages coordinate repair. Macrophages are essential for recruiting fibroblasts, stimulating angiogenesis, and producing the growth factors needed for tissue regeneration. Without adequate macrophage activity, repair is disorganized and incomplete.
Inflammatory signals guide regeneration. Many of the cytokines and growth factors produced during acute inflammation (including TGF-β, FGF, and PDGF) directly stimulate satellite cells, fibroblasts, and osteoblasts to begin rebuilding damaged tissue. Blocking these signals interferes with repair.
Research evidence: Multiple animal and human studies have shown that excessive early NSAID use can impair bone fracture healing, tendon repair, and muscle regeneration. This does not mean NSAIDs should never be used — they are valuable for pain management — but their use should be thoughtful and timed appropriately.
Chronic Inflammation: When the System Fails to Resolve
Acute inflammation is beneficial because it resolves — it is a time-limited response. Chronic inflammation occurs when the resolution mechanisms fail and the inflammatory process continues for weeks, months, or years. This is pathological and destructive.
Chronic inflammation is characterized by:
- Persistent macrophage and lymphocyte infiltration.
- Ongoing tissue destruction.
- Attempts at healing that produce fibrosis (excess scar tissue) rather than normal tissue regeneration.
- Elevated systemic inflammatory markers (CRP, ESR).
Conditions involving chronic inflammation include:
- Chronic tendinopathy: Persistent low-grade inflammatory process in tendons that fails to resolve to normal tissue.
- Osteoarthritis: Chronic synovial inflammation contributing to cartilage degradation.
- Rheumatoid arthritis: Autoimmune chronic synovitis.
- Chronic low back pain: Often associated with central sensitization and systemic low-grade inflammation.
Physical therapy addresses chronic inflammation through:
- Graded exercise: Properly dosed exercise has been shown to have anti-inflammatory systemic effects, reducing circulating inflammatory markers.
- Eccentric loading: Particularly effective in tendinopathy — appears to help shift the local tissue environment from chronic inflammation toward repair.
- Manual therapy: Shown to have local anti-inflammatory effects through multiple mechanisms.
- Education and lifestyle modification: Addressing obesity, poor sleep, and sedentary behavior — all of which promote chronic systemic inflammation.
The RICE Protocol: Evolving Evidence
For decades, RICE (Rest, Ice, Compression, Elevation) was the standard first-aid approach to acute soft tissue injuries. However, current evidence is more nuanced:
Rest: Complete rest is rarely optimal. Early controlled movement (within pain tolerance) is now preferred — it promotes normal tissue alignment, prevents excessive scar formation, and maintains cardiovascular fitness.
Ice (Cryotherapy): Ice reduces pain and swelling short-term but may slow healing if applied excessively by reducing blood flow and impeding the inflammatory response needed for repair. Current guidelines suggest using ice primarily for pain management rather than healing acceleration.
Compression: Remains valuable for controlling swelling and supporting venous/lymphatic return.
Elevation: Effective for reducing dependent edema.
Some clinicians now use the acronym PEACE & LOVE (Protection, Elevation, Avoid Anti-inflammatories, Compression, Education; Load, Optimism, Vascularization, Exercise) to reflect a more nuanced approach that respects the healing biology of inflammation.
Heat vs Cold: When to Use Which
A common question in physical therapy: should I use heat or ice?
- Ice (cold therapy): Best for acute injuries (first 48-72 hours) primarily for pain management. Reduces nerve conduction velocity (reducing pain signal intensity) and temporarily reduces swelling through vasoconstriction. Not recommended for muscle spasms or chronic pain.
- Heat (thermotherapy): Best for chronic pain, muscle spasms, and preparing tissue for exercise. Heat causes vasodilation, increases local blood flow, improves tissue extensibility, and reduces muscle guarding. Not appropriate for acute injuries with significant swelling.
This guidance is grounded directly in inflammation physiology: cold for acute inflammation management; heat for chronic pain and pre-exercise tissue preparation.
Conclusion
Inflammation is neither friend nor foe — it is a biological tool that is beneficial when used at the right time and in the right amount, and harmful when it persists unnecessarily. Physical therapy’s approach to inflammation is built on this understanding: support the acute inflammatory response by avoiding excessive suppression in the early stages, promote resolution through appropriate exercise and nutrition, and address chronic inflammation with targeted interventions that help the body finally complete the repair process that was interrupted.
Understanding inflammation empowers physical therapy patients to make better decisions about ice versus heat, medication timing, and the appropriate balance between activity and rest during recovery. It transforms a confusing, uncomfortable experience into a comprehensible and manageable biological process.
References
- Hall, J.E., & Hall, M.E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier.
- Costanzo, L.S. (2022). Physiology (7th ed.). Elsevier.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.