Platelets and Blood Clotting: How Wounds Heal and What It Means for Physical Therapy
Learn how platelets and the coagulation cascade stop bleeding, initiate healing, and how platelet biology informs physical therapy and PRP treatments.
Every injury that breaks blood vessels — from a minor skin abrasion to a surgical incision, from a muscle tear to a fractured bone — must be met with an immediate response: stop the bleeding. The body accomplishes this with remarkable speed and precision through a process called hemostasis, in which platelets (thrombocytes) and a cascade of clotting proteins work together to seal the breach. But platelets do far more than plug holes in vessels — they are also key initiators of tissue repair, carrying within their tiny granules a rich arsenal of growth factors that launch the entire healing process.
For physical therapy patients, understanding platelet biology helps explain the biological timeline of healing, why platelet-rich plasma (PRP) therapy is increasingly used alongside physical therapy, and how certain medications and health conditions affect recovery.
What Are Platelets?
Platelets are the smallest of the blood cells, measuring just 2–3 micrometers in diameter. They are not true cells — they are anucleate cell fragments, derived from large bone marrow cells called megakaryocytes. Each megakaryocyte produces thousands of platelets by shedding fragments of its cytoplasm.
The normal platelet count in adults is 150,000–400,000 per microliter of blood. A low platelet count (thrombocytopenia) impairs clotting and increases bleeding risk — a consideration in physical therapy for patients on anticoagulant medications or with blood disorders. A high count (thrombocytosis) can occur after surgery, inflammation, or iron deficiency.
Platelets are normally inactive as they circulate in the blood. They are activated rapidly when they contact damaged vessel walls — particularly exposed collagen (normally hidden beneath the intact endothelium) — or when they receive chemical signals from damaged tissue.
Hemostasis: The Three Phases of Stopping Bleeding
Hemostasis (from the Greek haima = blood, stasis = standing still) occurs in three overlapping phases:
Phase 1 — Vascular Spasm (Immediate)
Within seconds of vessel injury, the damaged vessel constricts reflexively — reducing blood flow through the injured area. This vascular spasm is triggered by damage to the vessel wall, pain signals, and chemicals released by platelets. While it slows blood loss, it is insufficient alone to permanently stop bleeding from all but the smallest vessels.
Phase 2 — Primary Hemostasis: The Platelet Plug (Minutes)
Platelet plug formation proceeds through three steps:
Platelet adhesion: Exposed collagen in the damaged vessel wall is recognized by von Willebrand factor (vWF) — a protein that acts as a bridge between collagen and platelet receptors (GPIb). Platelets adhere to the collagen-vWF complex.
Platelet activation: Adherent platelets become activated — they change shape (from discoid to spiky), increase their metabolic activity, and begin releasing the contents of their internal granules:
- Alpha granules contain clotting factors (fibrinogen, factor V), growth factors (PDGF, TGF-β, VEGF, EGF), and adhesion proteins.
- Dense granules contain ADP, serotonin, and calcium — which activate nearby platelets.
Platelet aggregation: Released ADP activates additional platelets, which aggregate (pile up) at the injury site, binding to each other through fibrinogen bridges mediated by integrin receptors (GPIIb/IIIa). This forms the platelet plug — a loose but effective initial barrier.
Phase 3 — Secondary Hemostasis: The Coagulation Cascade (Minutes)
The coagulation cascade is a series of enzymatic reactions in which clotting factors (numbered I–XIII) are activated sequentially, ultimately producing fibrin — a tough, insoluble protein that reinforces and stabilizes the platelet plug.
The cascade has two pathways:
- The extrinsic pathway (tissue factor pathway): Triggered by tissue factor (TF) expressed by cells outside the blood vessel when they are exposed by injury. TF binds to factor VII, initiating the cascade.
- The intrinsic pathway (contact activation pathway): Triggered by contact of blood with damaged vessel surfaces.
Both pathways converge on factor X, which (with cofactor V) converts prothrombin (factor II) to thrombin. Thrombin then converts soluble fibrinogen (factor I) into fibrin strands. Fibrin forms a mesh that traps more platelets and red blood cells, creating a stable clot.
Factor XIII (also activated by thrombin) cross-links fibrin strands, making the clot mechanically strong.
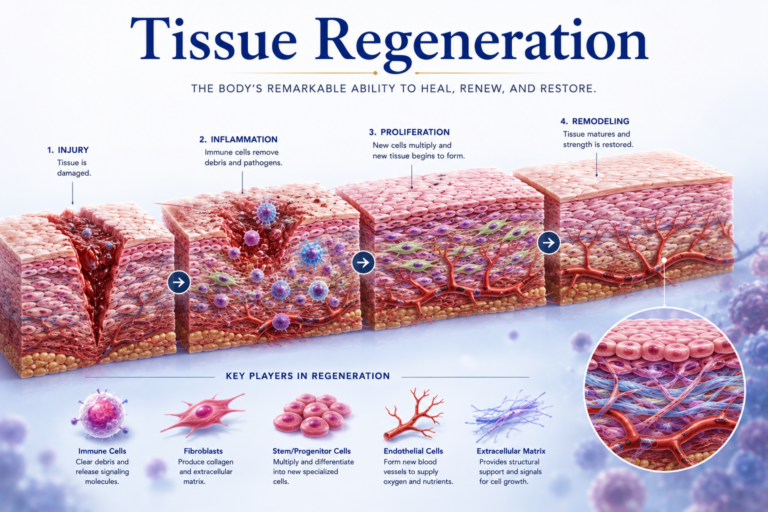
The Growth Factor Arsenal: Platelets as Initiators of Healing
Beyond their role in hemostasis, activated platelets release a remarkable array of growth factors that initiate the tissue repair cascade:
Platelet-Derived Growth Factor (PDGF): Stimulates fibroblast and smooth muscle cell proliferation; promotes new blood vessel formation (angiogenesis). One of the first signals to fibroblasts to begin collagen production.
Transforming Growth Factor-Beta (TGF-β): A multifunctional cytokine that stimulates collagen synthesis, promotes fibroblast differentiation, modulates the inflammatory response, and is involved in scar formation.
Vascular Endothelial Growth Factor (VEGF): Promotes angiogenesis — the growth of new blood vessels into the healing tissue. Essential for supplying the oxygen and nutrients needed for repair.
Epidermal Growth Factor (EGF): Stimulates epithelial cell proliferation — important for wound re-epithelialization.
Fibroblast Growth Factor (FGF): Promotes fibroblast proliferation and angiogenesis.
Insulin-Like Growth Factor 1 (IGF-1): Promotes cell proliferation, survival, and protein synthesis in multiple tissue types.
This rich growth factor cocktail explains why platelets are not just clotting tools — they are genuine biological initiators of healing. When a clot forms in a muscle tear, tendon injury, or bone fracture, the platelet granules begin releasing these growth factors, signaling surrounding cells to mobilize, proliferate, and begin building new tissue.
Platelet-Rich Plasma (PRP) Therapy
Platelet-rich plasma (PRP) is a preparation made from the patient’s own blood, in which platelets are concentrated (typically 3–8 times the normal concentration) by centrifugation and then injected into an injured tissue.
The rationale is straightforward: if platelets deliver growth factors that initiate healing, delivering more platelets to a sluggish or poorly healing tissue should accelerate the process.
PRP is used in orthopedic and sports medicine practice for conditions including:
- Chronic tendinopathies (Achilles, patellar, rotator cuff, lateral epicondyle)
- Osteoarthritis
- Muscle injuries
- Ligament sprains
Physical therapy is typically prescribed alongside PRP — providing the mechanical loading and progressive exercise that the growth factor-stimulated cells need to organize properly and produce high-quality tissue.
The evidence for PRP is still evolving. Results vary by condition, preparation method, and study quality. However, for chronic tendinopathy in particular, several high-quality studies show clinically meaningful benefits when PRP is combined with a structured physical therapy program.
Anticoagulants and Physical Therapy
Many physical therapy patients are on anticoagulant medications (blood thinners) — including warfarin, heparin, and newer oral anticoagulants (NOACs). These medications interfere with the coagulation cascade to reduce the risk of dangerous clot formation (deep vein thrombosis, pulmonary embolism, stroke).
For physical therapists, key considerations include:
- Increased bruising risk: Patients on anticoagulants bruise more easily and may develop larger hematomas after manual therapy or exercise-induced muscle trauma.
- Clotting time: Hemostasis after minor wounds or needle procedures (like dry needling) takes longer.
- Exercise safety: Vigorous exercise in anticoagulated patients requires assessment of injury risk, as significant bleeding from an injury is harder to control.
Physical therapists review patients’ medication lists and tailor their interventions accordingly — choosing techniques with lower bruising and impact risk when appropriate.
Conclusion
Platelets are small but mighty — the first responders to vessel injury, the constructors of the initial hemostatic plug, and the launchers of the tissue repair cascade through their remarkable growth factor payload. Understanding platelet biology illuminates the biology of healing at the earliest and most fundamental level.
For physical therapy patients, this knowledge is relevant whether they are recovering from an acute injury, managing a chronic tendinopathy potentially treatable with PRP, or navigating rehabilitation while on anticoagulant therapy. Platelets represent the moment where the body’s healing machinery first activates — and physical therapy provides the structured biological environment in which that machinery can do its best work.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.