The Immune System: How Your Body Defends Itself After Injury and During Physical Therapy
Learn how the immune system responds to injury, how it coordinates the healing process, and how physical therapy supports immune function during rehabilitation.
When you sprain an ankle, tear a muscle, or undergo surgery, your body faces a dual challenge: repair the damaged tissue and defend against potential infection. Both tasks fall to the immune system — a remarkably complex network of cells, proteins, and organs that works around the clock to maintain the body’s integrity. Far from being a simple defense mechanism, the immune system is the architect of the healing process, directing every stage of tissue repair from the initial inflammatory response to the final remodeling of new tissue.
For physical therapy patients and practitioners, understanding the immune system clarifies why certain therapeutic approaches work, why the timing of interventions matters, and why supporting overall health during rehabilitation — through sleep, nutrition, and stress management — is genuinely important for recovery.
The Two Arms of the Immune System
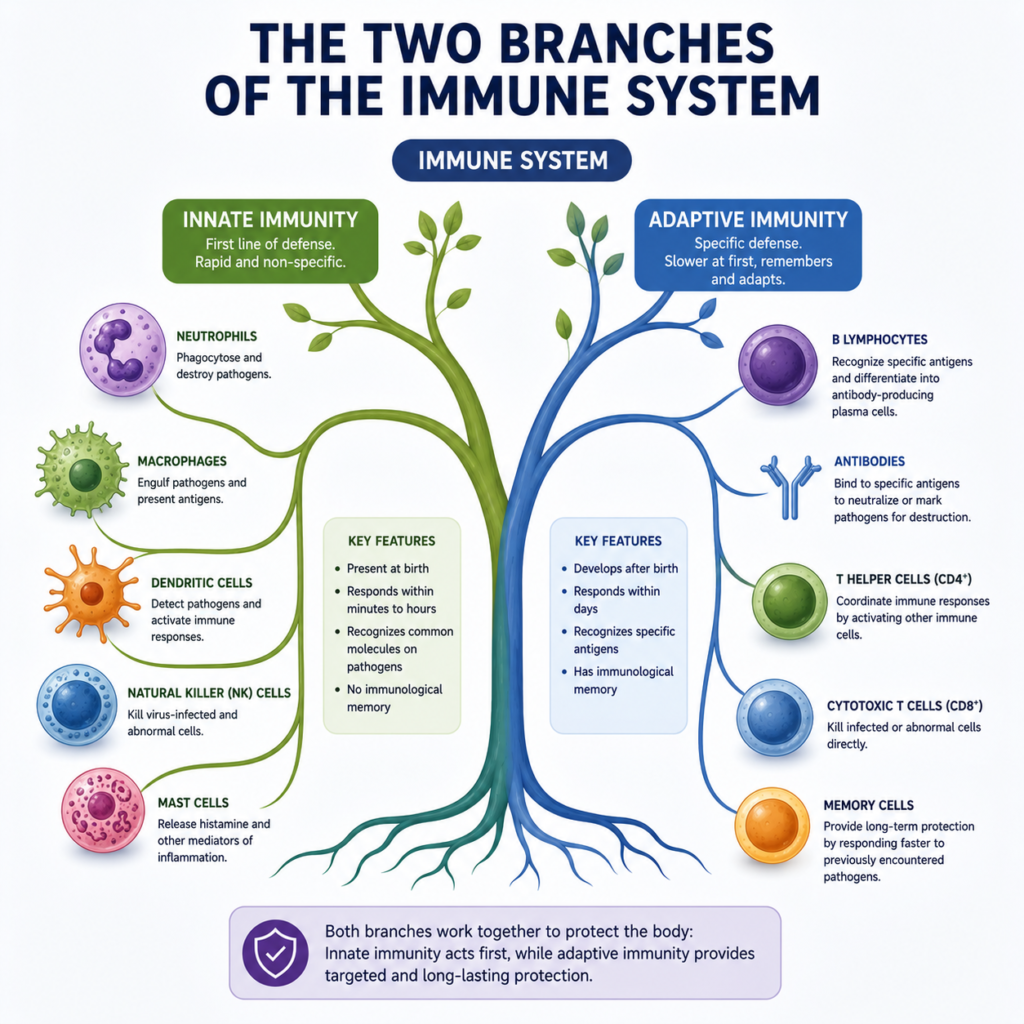
The immune system is divided into two broad components that work together:
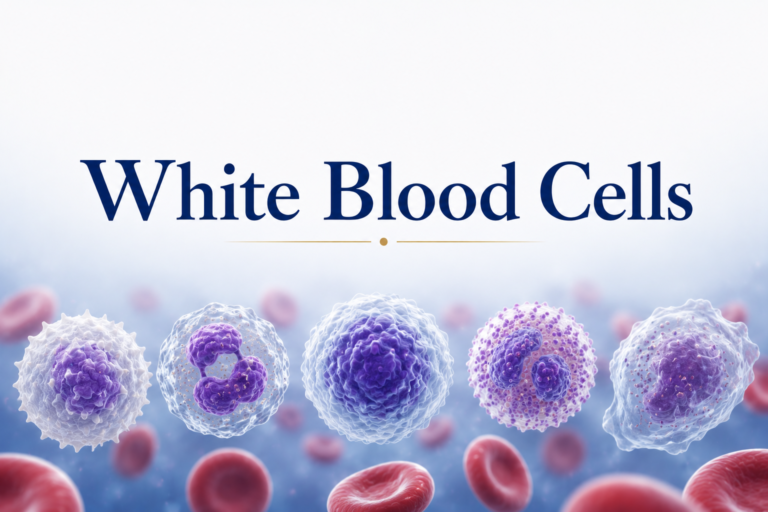
Innate immunity is the rapid, non-specific first line of defense. It responds within minutes to hours and does not require prior exposure to a pathogen or injury signal. Innate immune cells include neutrophils, macrophages, natural killer cells, dendritic cells, and mast cells. Physical barriers — skin, mucous membranes, respiratory cilia — are also considered part of innate immunity.
Adaptive immunity is the slower, highly specific system that develops over days to weeks after initial exposure. It involves B lymphocytes (which produce antibodies) and T lymphocytes (which directly kill infected cells and coordinate the immune response). Unlike innate immunity, adaptive immunity creates immunological memory — enabling a faster, stronger response upon re-exposure to the same pathogen.
In the context of musculoskeletal injury and physical therapy, innate immunity plays the dominant role. The adaptive immune system becomes more relevant in cases of infection, autoimmune conditions (like rheumatoid arthritis), and some chronic inflammatory conditions.
The Innate Immune Response to Tissue Injury
When tissue is injured — by trauma, surgery, or overuse — several simultaneous events activate the innate immune system:
Pattern recognition: Damaged cells release molecules called DAMPs (Damage-Associated Molecular Patterns) — including heat-shock proteins, fragments of DNA, and cellular contents like ATP and uric acid. These DAMPs are recognized by pattern recognition receptors (PRRs) on immune cells, signaling that damage has occurred.
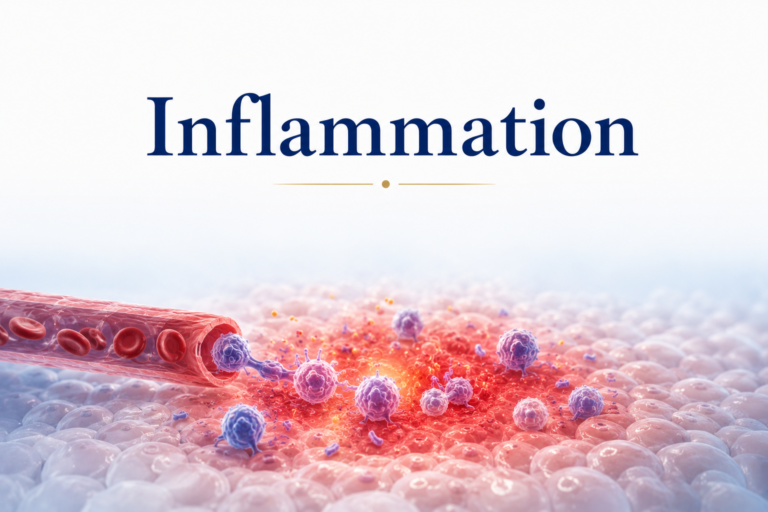
Mast cell activation: Mast cells resident in connective tissue detect injury signals and immediately release histamine and other pre-formed inflammatory mediators. Histamine causes local vasodilation (more blood to the area) and increased vascular permeability (allowing immune cells and proteins to leak into the tissue) — producing the classic signs of acute inflammation: redness (rubor), heat (calor), swelling (tumor), and pain (dolor).
Neutrophil infiltration: Within minutes to hours, neutrophils — the most abundant white blood cells — are recruited to the injury site by chemical signals (chemokines) and begin entering the tissue from blood vessels. Neutrophils engulf bacteria and cellular debris through phagocytosis and release enzymes that destroy pathogens. They are the first responders of the immune system.
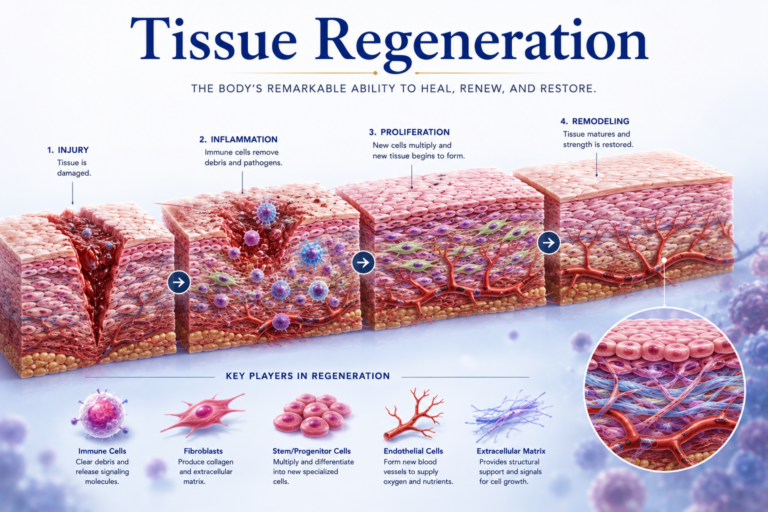
Macrophage arrival: Within 24-48 hours, monocytes arrive from the blood and differentiate into macrophages — more powerful phagocytes that can engulf larger debris and produce an extensive array of cytokines (signaling proteins). Macrophages perform several critical functions:
- Clearing apoptotic neutrophils and cellular debris (essential for resolving inflammation).
- Releasing growth factors (including TGF-β, PDGF, and FGF) that stimulate fibroblast activity and new blood vessel formation.
- Polarizing between pro-inflammatory (M1) and anti-inflammatory/repair-promoting (M2) phenotypes as healing progresses.
The transition from M1 to M2 macrophage dominance is a critical step in resolving inflammation and initiating repair. Physical therapy interventions — including gentle exercise and manual therapy — have been shown to influence this macrophage polarization.
Immune Cells and Specific Tissue Repair
Different tissues have different relationships with the immune system during repair:
Muscle: After muscle injury, neutrophils and macrophages infiltrate the tissue. Initially, they perform essential cleanup functions (removing damaged myofibers) that are necessary for regeneration. However, excessive or prolonged neutrophil activity can damage satellite cells and delay regeneration. Physical therapy exercises that promote gentle movement during the early phases of muscle healing help regulate the immune response without impeding it.
Tendon: Tendon healing is heavily dependent on macrophages. In acute tendon injuries, macrophage activity drives the initial repair response. In chronic tendinopathy, an aberrant, non-resolving immune response (characterized by persistent M1 macrophage activity and the presence of mast cells) contributes to the degenerative changes seen in the tendon. Eccentric exercise in physical therapy may help shift this immune environment toward resolution and repair.
Bone: Fracture healing is orchestrated in part by the immune system. Periosteal macrophages (osteomacs) are essential for normal fracture repair. Hematoma formation and the initial inflammatory response are necessary precursors to the callus formation that eventually repairs the fracture. Premature suppression of this inflammatory response — such as with high-dose NSAIDs used too early — may impair fracture healing.
The Resolution of Inflammation: An Active Process
For many years, the resolution of inflammation was assumed to be a passive process — the natural consequence of inflammatory mediators being diluted and eliminated. Modern immunology has revealed that resolution is in fact an active, highly regulated process requiring specific molecules called specialized pro-resolving mediators (SPMs).
SPMs — including resolvins (derived from omega-3 fatty acids EPA and DHA), protectins, and lipoxins — actively signal macrophages to stop producing pro-inflammatory cytokines, begin clearing debris, and initiate tissue repair. They are produced in increasing quantities as inflammation progresses.
This understanding has several clinical implications for physical therapy:
- Omega-3 fatty acid intake supports SPM production and may accelerate the resolution of inflammation.
- Excessive use of NSAIDs (which block the prostaglandin pathway) may also reduce production of certain SPMs (derived from the same pathway), potentially slowing resolution.
- Physical exercise stimulates SPM production — providing an anti-inflammatory benefit that goes beyond simple pain relief.
Exercise and Immune Function
Regular moderate exercise has well-documented immunological benefits:
- Enhanced natural killer cell activity.
- Improved macrophage function.
- Increased antibody production.
- Reduced chronic systemic inflammation (lower CRP, IL-6, and TNF-α in sedentary individuals who begin exercising).
These benefits are relevant to physical therapy rehabilitation: patients who maintain active exercise programs not only heal musculoskeletal injuries faster but also have lower rates of post-surgical infection and improved systemic health markers.
However, excessive exercise — particularly in untrained individuals or following intense rehabilitation sessions — can temporarily suppress immune function (the “open window” of immunosuppression) lasting 3-24 hours after very intense exercise. This explains why adequate recovery between intense sessions is important.
Autoimmune Conditions and Physical Therapy
When the immune system mistakenly attacks the body’s own tissues, autoimmune disease results. Conditions like rheumatoid arthritis (attacking joint synovium), lupus, ankylosing spondylitis, and psoriatic arthritis are frequently managed with physical therapy.
Physical therapy in autoimmune musculoskeletal conditions aims to:
- Maintain joint range of motion during flares through gentle, pain-free exercise.
- Strengthen muscles supporting affected joints.
- Reduce secondary complications (contractures, deformities, cardiovascular deconditioning).
- Educate patients about activity modification and joint protection strategies.
The systemic anti-inflammatory effects of regular moderate exercise benefit autoimmune patients significantly — reducing disease activity markers and improving quality of life alongside medical management.
Conclusion
The immune system is the body’s guardian and architect — defending against infection, coordinating the healing response, and ensuring that injured tissues are rebuilt properly. In physical therapy, understanding immune physiology explains why the timing of interventions matters (respecting the phases of healing), why supporting immune function through nutrition, sleep, and stress management accelerates recovery, and why therapeutic exercise itself has anti-inflammatory effects.
Rather than working around the immune system, effective physical therapy works with it — supporting the innate responses that are essential for healing while helping to resolve excessive inflammation and guide tissues toward optimal repair and remodeling.
References
- Hall, J.E., & Hall, M.E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier.
- Punt, J., Stranford, S., Jones, P., & Owen, J. (2018). Kuby Immunology (8th ed.). W.H. Freeman.
- Costanzo, L.S. (2022). Physiology (7th ed.). Elsevier.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.