Body Fluids: Intracellular vs Extracellular and Their Role in Edema Management
Understand how body fluid compartments work, what causes edema after injury or surgery, and how physical therapy techniques manage fluid balance to support healing.
Swelling after an injury is one of the most immediately visible signs that something has gone wrong in the body. It is also one of the most common challenges managed in physical therapy. Whether it follows a sprained ankle, a surgical procedure, a fracture, or a lymphatic disorder, edema — the pathological accumulation of fluid in tissue — impairs movement, causes pain, and slows the healing process.
Understanding why edema occurs requires understanding how fluid is normally distributed in the body, what forces govern its movement, and how physical therapy interventions can restore normal fluid dynamics. This is not merely academic — it directly informs some of the most effective physical therapy techniques for managing swelling.
Body Fluid Compartments
The human body is approximately 60% water by weight — around 42 liters in a 70-kg adult. This fluid is distributed between two main compartments, separated by cell membranes:
Intracellular fluid (ICF): Approximately two-thirds of body water (28 liters) is found inside cells. This fluid contains high concentrations of potassium (K⁺), magnesium (Mg²⁺), and phosphate ions, along with proteins and other organic molecules. It is the aqueous medium in which all cellular reactions take place.
Extracellular fluid (ECF): The remaining one-third (14 liters) is outside cells. ECF is further divided into:
- Interstitial fluid (approximately 11 liters): The fluid that directly bathes cells in tissues. It acts as the intermediary between blood and cells — oxygen and nutrients diffuse from blood into interstitial fluid, and cells absorb what they need from it.
- Plasma (approximately 3 liters): The liquid component of blood within blood vessels.
- Transcellular fluid (approximately 1 liter): Specialized fluids including synovial fluid, cerebrospinal fluid, and aqueous humor.
The composition of ICF and ECF differs significantly, and maintaining these differences is essential for normal cell function. The Na⁺/K⁺-ATPase pump in cell membranes actively maintains these gradients by pumping 3 sodium ions out and 2 potassium ions in, consuming ATP.
Starling Forces: What Controls Fluid Movement
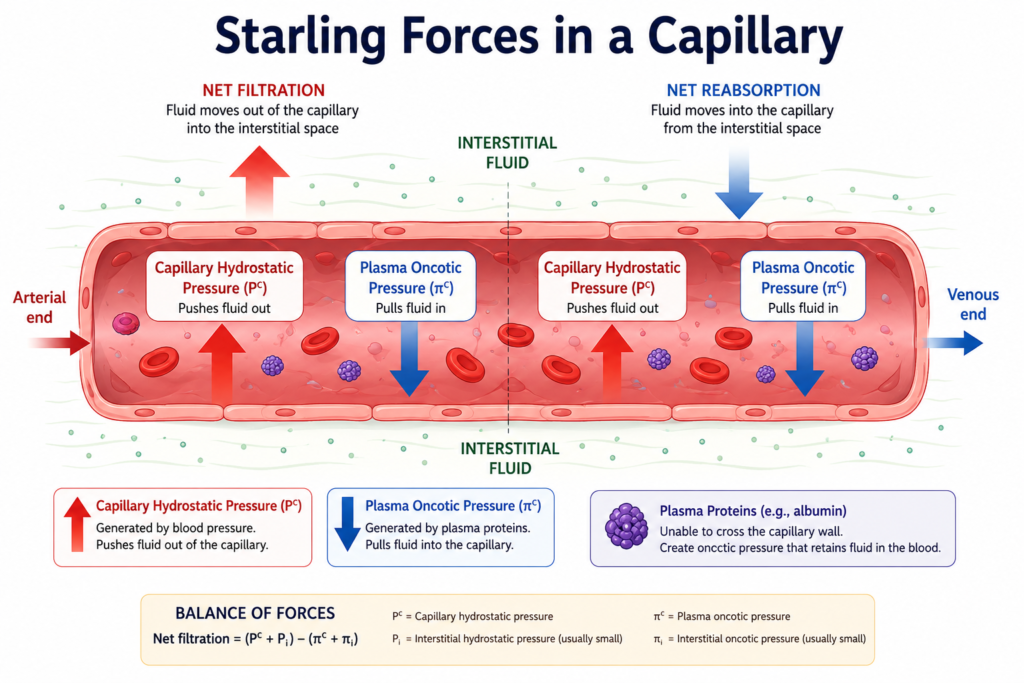
Fluid moves between the bloodstream and interstitial space across capillary walls — thin, semi-permeable membranes. The direction and volume of this movement are determined by four opposing forces, collectively known as Starling forces:
1. Capillary hydrostatic pressure (Pc): The pressure of blood within capillaries pushes fluid outward into the interstitial space. This is highest at the arterial end of a capillary (approximately 35 mmHg) and falls to about 15 mmHg at the venous end.
2. Interstitial hydrostatic pressure (Pi): The pressure of fluid already in the interstitial space, which opposes further outward movement. Under normal conditions, this is close to zero or slightly negative (slightly sub-atmospheric), which actually helps fluid move out of capillaries.
3. Plasma oncotic pressure (πc): Proteins in the blood (primarily albumin) exert an osmotic force that pulls fluid back into the capillary — approximately 25 mmHg. This is the main force opposing outward filtration.
4. Interstitial oncotic pressure (πi): Proteins in the interstitial fluid attract water, opposing return to the capillary — approximately 5 mmHg.
At the arterial end of capillaries, the net effect of these forces favors filtration (fluid moves outward). At the venous end, the net effect favors reabsorption (fluid moves back in). The small amount of fluid that is not reabsorbed at the venous end is collected by the lymphatic system and returned to the bloodstream.
Under normal conditions, this system is finely balanced. Edema develops when any of these forces is disrupted.
Causes of Edema Relevant to Physical Therapy
Physical therapy patients encounter several common causes of edema:
Increased capillary hydrostatic pressure: In venous insufficiency (where veins fail to return blood efficiently to the heart), venous pressure backs up into capillaries, increasing capillary hydrostatic pressure and driving fluid into tissues. This produces dependent edema — swelling in the feet and ankles that worsens with prolonged standing and improves with elevation.
Increased capillary permeability: During the inflammatory response to injury, mediators like histamine, bradykinin, and prostaglandins increase capillary permeability, allowing protein-rich fluid to leak into the interstitial space. This inflammatory edema is the warm, tender swelling seen immediately after an acute injury — the body’s necessary but uncomfortable first step in healing.
Reduced plasma oncotic pressure: If blood protein (particularly albumin) levels are low — due to malnutrition, liver disease, or kidney disease — the oncotic pressure pulling fluid back into capillaries is reduced, allowing fluid to accumulate in tissues. This is one reason why adequate protein intake is important in rehabilitation patients with complex medical histories.
Impaired lymphatic drainage: The lymphatic system is responsible for collecting excess interstitial fluid and returning it to the bloodstream. If lymphatic vessels are damaged or removed — as happens after cancer surgery involving lymph node dissection — fluid accumulates permanently, a condition called lymphedema. This is a major focus of specialized physical therapy.
Post-surgical and post-traumatic edema: After surgery or injury, all of the above mechanisms can operate simultaneously. Tissue damage increases capillary permeability; the inflammatory response drives fluid outward; and reduced mobility impairs the muscular pumping action that assists lymphatic and venous return.
Physical Therapy Interventions for Edema Management
Physical therapy has a well-established toolkit for managing edema:
Elevation: Raising an injured limb above the level of the heart uses gravity to facilitate venous and lymphatic return, reducing capillary hydrostatic pressure and the net outward filtration force. Patients are commonly instructed to elevate injured limbs whenever possible in the early days after injury or surgery.
Compression therapy: Elastic compression bandages or garments increase interstitial hydrostatic pressure and support venous and lymphatic return. Compression therapy is a cornerstone of lymphedema management and post-surgical swelling control.
Active exercise: Muscle contractions act as a pump for both venous and lymphatic systems. Every muscle contraction squeezes lymphatic and venous vessels, propelling fluid toward the central circulation. This is one reason why early mobilization — even gentle active range-of-motion exercises — is encouraged after injury and surgery: it combats fluid accumulation.
Manual lymphatic drainage (MLD): A specialized massage technique that uses very light, rhythmic strokes to stimulate lymphatic vessel contraction and redirect lymphatic flow around blocked or damaged areas. Used primarily in lymphedema management.
Pneumatic compression: Sequential compression devices (inflatable sleeves that apply cyclic pressure) mechanically assist venous and lymphatic return — particularly useful for patients who cannot perform adequate active exercise.
Electrolytes and Fluid Balance
The distribution of water between body compartments is governed by osmosis — water moves across semi-permeable membranes toward areas of higher solute concentration. Electrolytes (sodium, potassium, chloride) are the primary determinants of osmolarity in each compartment.
Sodium is the dominant cation in extracellular fluid. When sodium levels rise (from excessive salt intake, dehydration, or hormonal imbalance), water is retained in the extracellular compartment, increasing blood volume and pressure. When sodium levels fall, water moves into cells (potentially causing cellular swelling).
Physical therapy patients who are dehydrated have reduced plasma volume, impairing the cardiovascular system’s ability to deliver oxygen and nutrients to healing tissues. Maintaining adequate hydration is therefore essential during rehabilitation.
Conclusion
The body’s fluid compartments are precisely regulated systems. When injury, surgery, inflammation, or disease disrupts this regulation, edema results — impairing movement, causing pain, and slowing the healing process. Physical therapy provides a scientifically grounded set of interventions — elevation, compression, exercise, manual drainage, and education — that work with the body’s natural fluid management systems to restore balance.
Understanding the physiology of body fluids helps both therapists and patients appreciate why these techniques work and why consistent application of fluid management strategies is an important part of comprehensive rehabilitation.
References
- Hall, J.E., & Hall, M.E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier.
- Costanzo, L.S. (2022). Physiology (7th ed.). Elsevier.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.