Catabolism vs Anabolism: Understanding the Body’s Build and Break Cycle in Physical Therapy
Learn the difference between catabolism and anabolism, how these metabolic states affect muscle growth and tissue repair, and how physical therapy balances both for optimal recovery.
The human body is never static. Even when you are sitting still, your cells are engaged in a constant, dynamic interplay of building and breaking down — constructing new molecules, tearing apart old ones, extracting energy from nutrients, and using that energy to rebuild. This continuous cycle of construction and destruction is called metabolism, and it is divided into two broad, opposing phases: catabolism and anabolism.
For physical therapy patients, understanding this fundamental metabolic cycle is far more than an academic exercise. It explains why exercise is essential for tissue repair (not despite causing damage, but because of it), why rest is necessary for growth, why nutrition timing matters, and how therapeutic interventions are designed to shift the body toward a state of healing and regeneration.
Metabolism: The Sum of All Chemical Reactions
Metabolism refers to the complete set of chemical reactions occurring in the body at any given time. These reactions serve two fundamental purposes:
- Extracting energy from nutrients (food) to fuel biological work.
- Synthesizing the molecules the body needs — including structural proteins, enzymes, hormones, and nucleic acids.
Metabolism is exquisitely regulated. Cells receive signals — from hormones, nutrient availability, energy status, and mechanical forces — that determine which metabolic pathways are active at any moment. This regulation allows the body to adapt to feeding, fasting, exercise, injury, and recovery.
Catabolism: Breaking Down to Build Up
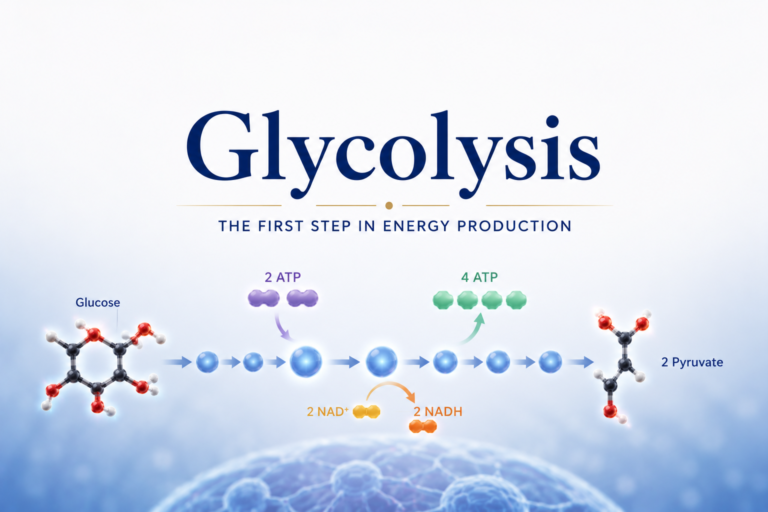
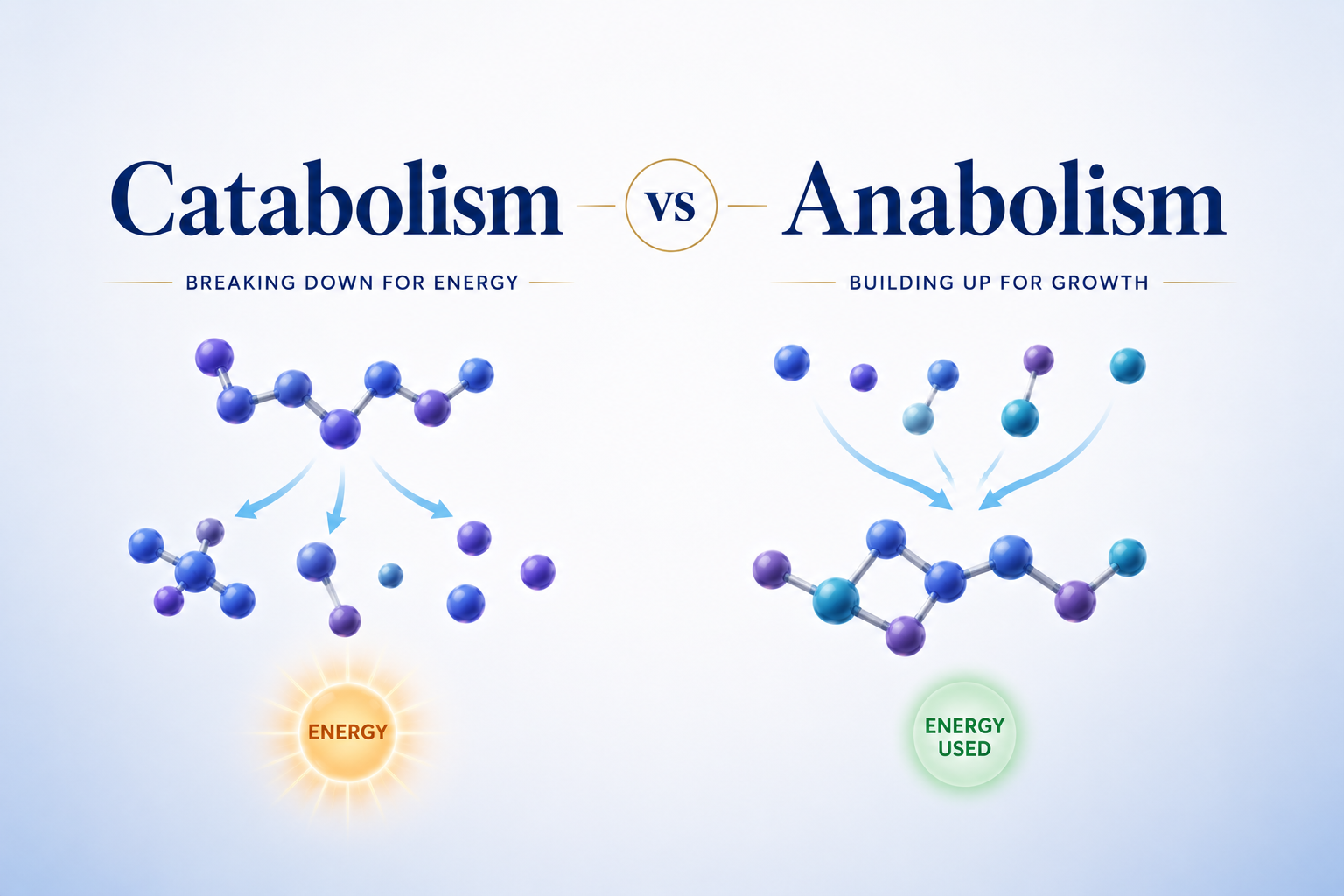
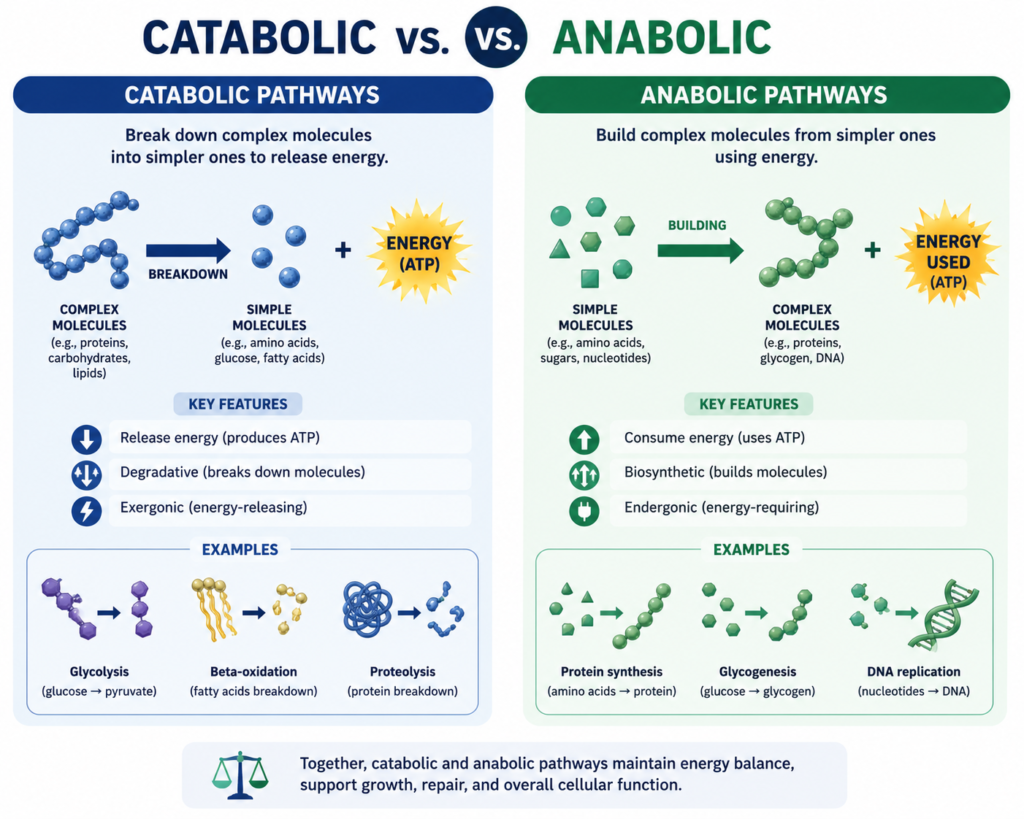
Catabolism encompasses all the metabolic reactions that break down complex molecules into simpler ones, releasing energy in the process. Catabolic pathways are exergonic — they release more energy than they consume.
Common catabolic processes include:
- Glycolysis: Breaking down glucose into pyruvate.
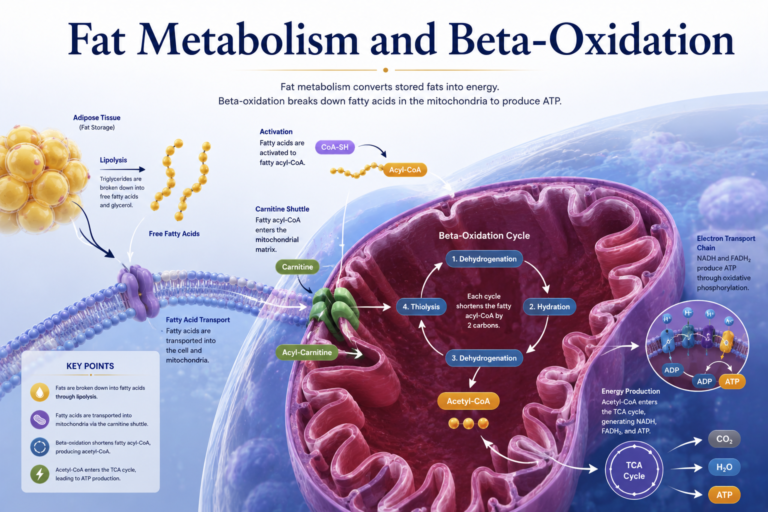
- Beta-oxidation: Breaking down fatty acids into acetyl-CoA.
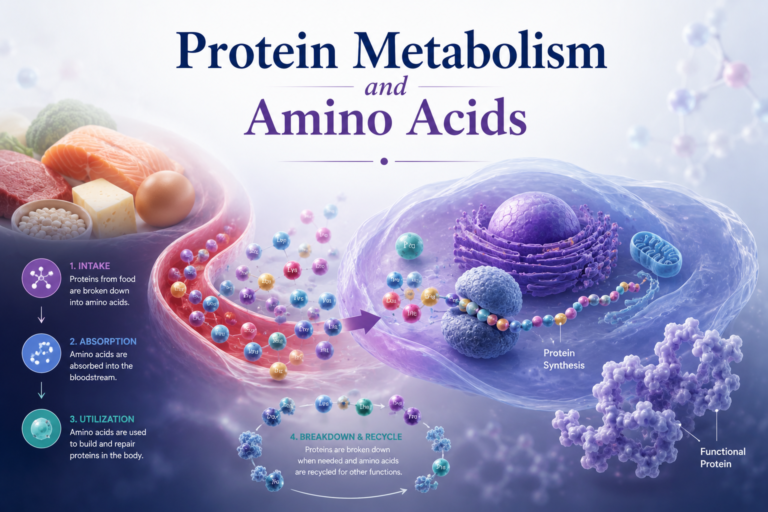
- Protein catabolism: Breaking down proteins (including muscle proteins) into amino acids.
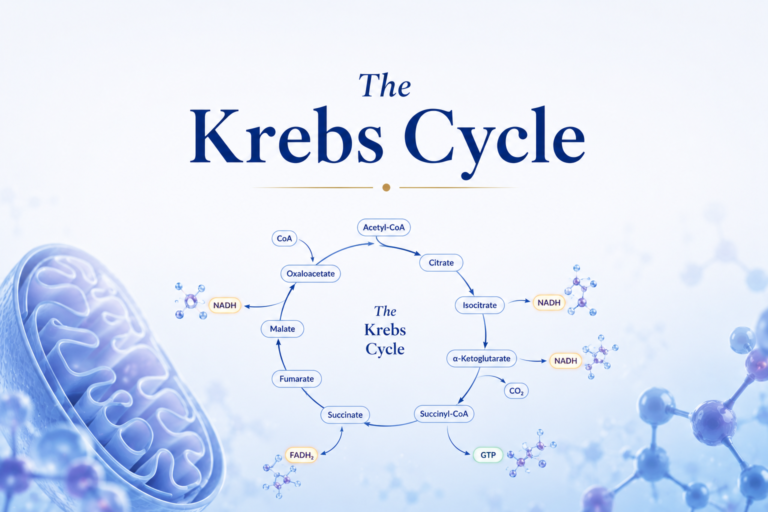
- The Krebs cycle: Oxidizing acetyl-CoA to CO₂, generating electron carriers.
- Bone resorption: Osteoclasts breaking down bone matrix to release calcium.
Catabolism is not inherently harmful — it is essential. Without it, the body could not extract energy from food, clear damaged cellular components, or remodel tissues. However, excessive or uncontrolled catabolism — such as the muscle protein breakdown seen during prolonged immobilization, illness, or severe caloric restriction — is destructive and must be managed carefully during rehabilitation.
Key catabolic hormones include:
- Cortisol (the primary stress hormone): Promotes protein breakdown in muscle and glucose mobilization. Released in response to physical stress, psychological stress, injury, and surgery.
- Glucagon: Released during fasting; promotes glycogen breakdown and gluconeogenesis.
- Epinephrine (adrenaline): Released during acute stress; rapidly mobilizes glucose and fatty acids.
Anabolism: Building the Body’s Structures
Anabolism encompasses all the metabolic reactions that build complex molecules from simpler precursors, using energy in the process. Anabolic pathways are endergonic — they consume more energy than they release, requiring ATP.
Common anabolic processes include:
- Protein synthesis: Building muscle proteins, enzymes, and structural proteins like collagen from amino acids.
- Glycogenesis: Storing glucose as glycogen in the liver and muscles.
- Lipogenesis: Converting excess nutrients into triglycerides for storage in adipose tissue.
- Bone formation: Osteoblasts building new bone matrix.
- DNA and RNA synthesis: Replication and transcription of genetic material.
Anabolism is the process by which the body repairs injured tissue, builds muscle, increases bone density, and restores strength after illness or injury. It is, quite literally, the biology of recovery.
Key anabolic hormones include:
- Insulin: Released after eating; promotes glucose uptake, protein synthesis, and glycogen storage.
- Growth hormone (GH): Stimulates growth and cell reproduction; promotes protein synthesis and fat oxidation.
- IGF-1 (Insulin-like Growth Factor 1): Mediates many of growth hormone’s anabolic effects in muscle and bone.
- Testosterone and estrogen: Promote muscle protein synthesis and bone mineralization.
The Catabolic-Anabolic Cycle: Why Exercise Works
One of the most important and counterintuitive concepts in exercise physiology is that therapeutic exercise induces both catabolism and anabolism — and this alternation is what drives adaptation.
During exercise, catabolic processes dominate:
- Glycogen is broken down to fuel muscle contraction.
- Muscle proteins are damaged (particularly during eccentric exercise).
- Cortisol and epinephrine levels rise.
- Oxidative stress increases.
During recovery after exercise, anabolic processes predominate:
- Growth hormone and testosterone rise.
- Insulin sensitivity increases, facilitating nutrient uptake.
- Muscle protein synthesis (MPS) accelerates significantly.
- Glycogen stores are rebuilt.
- Damaged proteins are cleared and replaced.
The net effect of this cycle — stress followed by recovery — is adaptation: stronger, more resilient muscle, denser bone, more efficient energy metabolism. Physical therapy exploits this cycle deliberately, applying controlled stress through therapeutic exercise and then supporting recovery through rest, nutrition, and appropriate modalities.
Muscle Protein Balance: The Anabolic-Catabolic Tipping Point
Muscle mass is determined by the balance between muscle protein synthesis (MPS) and muscle protein breakdown (MPB). When MPS > MPB, muscle grows. When MPB > MPS, muscle is lost. When they are equal, muscle mass is maintained.
Several factors shift this balance:
Exercise: Resistance exercise acutely increases both MPS and MPB, but MPS rises more, resulting in net muscle growth if protein intake is adequate.
Protein intake: Consuming protein — particularly leucine-rich proteins — powerfully stimulates MPS through the mTOR signaling pathway. A common recommendation for rehabilitation patients is 1.6-2.0 g of protein per kg of body weight per day.
Caloric intake: Severe caloric restriction tilts the balance toward catabolism — the body breaks down muscle for fuel. This is a concern during illness, surgery recovery, or extreme dieting combined with physical therapy.
Hormonal environment: High cortisol (from stress, injury, or poor sleep) drives MPB. High testosterone and IGF-1 drive MPS. Physical therapy patients can support their hormonal environment by managing stress, ensuring adequate sleep, and following a balanced diet.
Immobilization: Lack of mechanical loading rapidly tilts the balance toward catabolism. Even 5-7 days of bed rest or immobilization produces significant muscle loss. Early mobilization in physical therapy — even gentle range-of-motion exercises — helps counteract this catabolic response.
Practical Applications for Physical Therapy
Understanding catabolism and anabolism helps physical therapy patients make better decisions:
Match nutrition to training phase. During active rehabilitation, increase protein and calorie intake to support anabolism. During periods of reduced activity (due to pain flare-ups or fatigue), be cautious about maintaining caloric intake that could lead to fat gain without supporting muscle.
Sleep is anabolic. Growth hormone is predominantly secreted during deep sleep. Adequate sleep (7-9 hours) is essential for anabolism and recovery. Poor sleep elevates cortisol (catabolic) and reduces GH secretion (anabolic) — a double metabolic disadvantage for rehabilitation.
Manage stress to reduce cortisol. Chronic psychological stress chronically elevates cortisol, promoting catabolism. Mindfulness, relaxation strategies, and addressing psychosocial factors in rehabilitation help create a more anabolic internal environment.
Progressive overload drives adaptation. The catabolic stimulus (exercise stress) must be progressively increased to continue driving adaptation. Physical therapy programs that are too easy create insufficient catabolic stimulus; those that are too hard create excessive catabolism without adequate recovery — both limiting progress.
Conclusion
Catabolism and anabolism are not opposing enemies — they are complementary partners in the continuous dance of biological adaptation. Physical therapy is, at its metabolic core, a process of strategically applying catabolic stress (exercise) and then supporting anabolic recovery (rest, nutrition, sleep) in a progressive cycle that gradually rebuilds strength, function, and quality of life.
Understanding this cycle empowers patients to see their rehabilitation not as a series of exercises, but as a carefully managed metabolic strategy. Every workout, every rest day, every meal, and every night of sleep is a piece of the metabolic puzzle that leads to recovery.
References
- Nelson, D.L., & Cox, M.M. (2021). Lehninger Principles of Biochemistry (8th ed.). W.H. Freeman.
- Berg, J.M., Tymoczko, J.L., Gatto, G.J., & Stryer, L. (2019). Biochemistry (9th ed.). W.H. Freeman.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.