Connective Tissue: The Most Important Tissue in Physical Therapy
Understand how connective tissue — including tendons, ligaments, cartilage, and fascia — works and heals, and why it is the primary focus of physical therapy treatment.
If there is one tissue that physical therapists work with more than any other, it is connective tissue. Tendons, ligaments, cartilage, fascia, joint capsules, intervertebral discs — all of these structures are made of connective tissue. They are also among the most commonly injured, and their repair requires carefully designed physical therapy programs.
Yet connective tissue is often misunderstood. Many people think of it as a passive, structural material — little more than biological glue that holds the body together. In reality, connective tissue is a dynamic, metabolically active system that constantly remodels in response to mechanical forces, hormonal signals, and nutritional inputs. Understanding this system is key to understanding how physical therapy achieves its results.
What Is Connective Tissue?
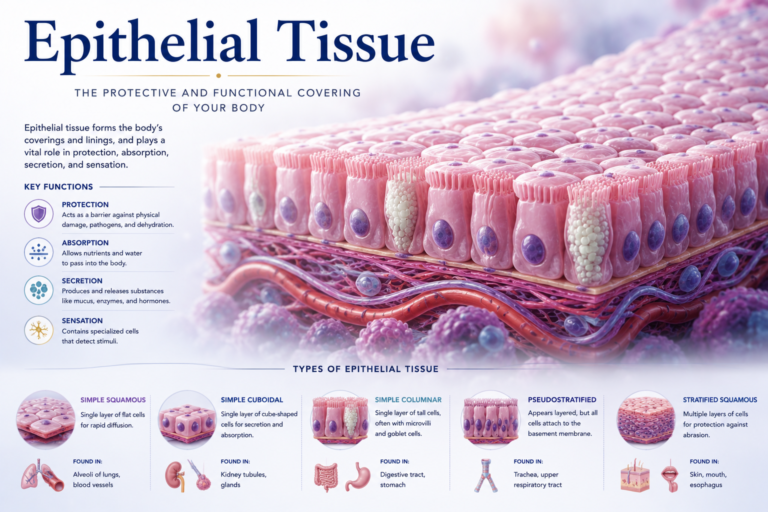
Connective tissue is characterized by three components:
- Cells — such as fibroblasts, chondrocytes, osteoblasts, or adipocytes, depending on the tissue type.
- Protein fibers — primarily collagen and elastin.
- Ground substance — a gel-like material that surrounds the fibers and cells, composed of water, proteoglycans, and glycoproteins.
The combination and arrangement of these components determine the mechanical properties of each connective tissue type. Dense, parallel collagen bundles give tendons their impressive tensile strength. The high water content of cartilage provides compressive resistance. The cross-linked elastin in ligaments allows elastic recoil.
Collagen: The Structural Backbone
Collagen is the most abundant protein in the human body, making up approximately 30% of total body protein. It is the primary structural molecule of most connective tissues and comes in many forms — at least 28 types have been identified.
Type I collagen is the most common and is found in tendons, ligaments, skin, and bone. It provides tensile strength — resistance to pulling forces.
Type II collagen is the main collagen in cartilage, where its unique structure helps resist compressive loads.
Type III collagen is found in skin, blood vessels, and organs, and also in early scar tissue. It is more flexible than Type I but less strong.
Collagen is produced by fibroblasts through a complex, multi-step process that requires specific nutrients — notably vitamin C (for a critical chemical modification called hydroxylation), zinc, copper, and adequate protein. Deficiencies in these nutrients impair collagen synthesis and slow tissue repair.
In physical therapy, one of the central goals during the remodeling phase of healing is to support the production of well-organized, high-quality collagen. Progressive mechanical loading guides fibroblasts to align new collagen fibers along lines of stress, improving the tensile strength and function of the repaired tissue.
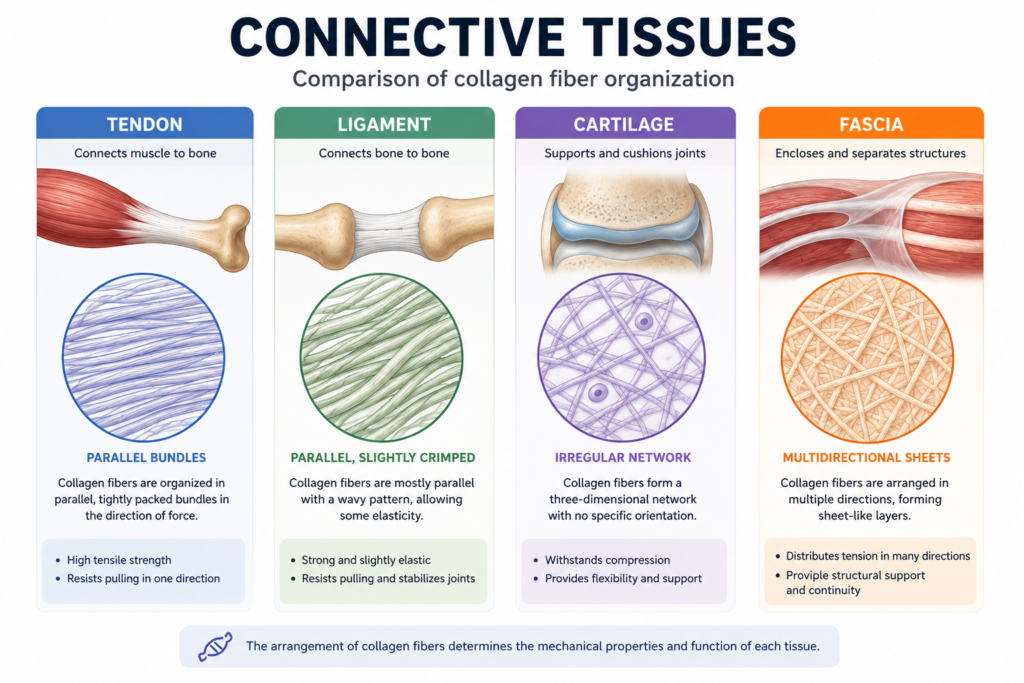
Tendons: Connecting Muscle to Bone
Tendons are dense connective tissue structures that transmit the force generated by muscles to the bones they move. They are composed primarily of tightly packed, parallel Type I collagen bundles arranged in a hierarchical structure from individual collagen molecules up to the whole tendon.
Tendons have a relatively poor blood supply compared to muscle, which is one reason they heal more slowly. They receive nutrition partly through direct blood vessels and partly through diffusion from synovial fluid in tendons enclosed by synovial sheaths.
Tendon cells (tenocytes) are fibroblasts specialized for tendon maintenance. They are sensitive to mechanical loading and respond to tension by upregulating collagen production and remodeling activity. This is the biological basis for progressive loading programs in tendon rehabilitation — without mechanical stimulus, tenocytes become less active and the tendon loses its structural integrity.
Common tendon conditions treated in physical therapy include Achilles tendinopathy, rotator cuff tendinopathy, patellar tendinopathy (jumper’s knee), and lateral epicondylalgia (tennis elbow). Exercise-based programs — particularly eccentric and heavy slow resistance training — have become the gold standard treatment for most tendinopathies.
Ligaments: Joint Stability and Proprioception
Ligaments connect bone to bone and provide passive stability to joints. Like tendons, they are composed primarily of Type I collagen, but with a less parallel arrangement that allows them to resist forces from multiple directions.
Ligament injuries — commonly called sprains — are graded by severity. Grade I involves minor stretching without structural damage. Grade II involves partial tearing. Grade III involves complete rupture. Physical therapy management differs significantly across these grades.
Beyond their mechanical role, ligaments contain proprioceptive nerve endings — sensory receptors that provide information about joint position and movement. Ligament sprains disrupt these nerve endings, impairing proprioception and increasing the risk of re-injury. Physical therapy programs for ligament injuries therefore include balance training, coordination exercises, and neuromuscular re-education — not just strength and range-of-motion work.
Cartilage: The Joint Cushion
Articular cartilage covers the ends of bones in synovial joints. It provides a smooth, low-friction surface for joint movement and acts as a shock absorber, distributing compressive loads across the joint surface.
Cartilage is composed of chondrocytes (cartilage cells) embedded in a matrix of Type II collagen and proteoglycans — large molecules that attract and hold water, giving cartilage its compressive resilience. A healthy adult articular cartilage is approximately 70-80% water.
The notoriously poor healing capacity of cartilage stems from two factors: it lacks blood vessels (it is avascular) and has very few cells with limited division capacity. This means that significant cartilage damage — as in osteoarthritis or traumatic cartilage lesions — rarely heals spontaneously.
Physical therapy for cartilage conditions focuses on managing compressive load on the joint, maintaining range of motion and muscle strength, reducing pain, and slowing the progression of degeneration. Aquatic therapy (hydrotherapy) is particularly valuable because it allows exercise with greatly reduced joint loading.
Fascia: The Body’s Hidden Connective Network
Fascia is a network of connective tissue that surrounds and connects all structures in the body — muscles, tendons, organs, bones, nerves, and blood vessels. It is a continuous sheet that extends from the top of the head to the tips of the toes.
Historically underappreciated, fascia is now recognized as a major contributor to movement efficiency, force transmission, and pain. Fascial restrictions — areas where the fascia becomes thickened, adhered, or dehydrated — can limit movement, alter muscle activation patterns, and generate pain.
Physical therapy techniques including myofascial release, soft tissue mobilization, foam rolling, and stretching all target the fascial system. These interventions are thought to improve fascial hydration, reduce mechanical restrictions, and normalize the sensory input from fascial mechanoreceptors.
How Mechanical Loading Remodels Connective Tissue
One of the most important principles in connective tissue rehabilitation is Wolff’s Law (for bone) and its connective tissue equivalent: connective tissue adapts its structure and strength in response to the mechanical loads placed upon it.
Under appropriate loading, fibroblasts increase collagen production and orient new fibers along lines of stress. Blood vessel ingrowth improves nutrient supply. Proteoglycan content increases, enhancing tissue hydration and resilience.
Without loading — during immobilization or prolonged inactivity — the opposite occurs: collagen degrades, fibers become randomly organized, and tissue loses tensile strength. This is why early, controlled movement is generally preferred over complete rest in modern connective tissue rehabilitation.
Conclusion
Connective tissue is the structural foundation of the musculoskeletal system and the primary focus of most physical therapy interventions. From the collagen fibers of a repairing tendon to the proteoglycans of a loaded cartilage surface, every aspect of connective tissue biology responds to the mechanical and therapeutic environment created by physical therapy.
Understanding connective tissue means understanding why progressive loading works, why early movement matters, and why nutrition supports healing. It transforms physical therapy from a set of exercises into a scientifically grounded approach to tissue biology — one that works with the body’s own mechanisms to restore structure, function, and quality of life.
References
- Ross, M.H., & Pawlina, W. (2020). Histology: A Text and Atlas (8th ed.). Wolters Kluwer.
- Mescher, A.L. (2021). Junqueira’s Basic Histology: Text and Atlas (16th ed.). McGraw-Hill.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.