Fat Metabolism and Beta-Oxidation: Low-Intensity Exercise and Recovery in Physical Therapy
Learn how the body burns fat through beta-oxidation, why low-intensity exercise maximizes fat use, and how fat metabolism supports physical therapy recovery programs.
“Burn fat, not sugar” — a phrase often heard in fitness circles. But what does it actually mean biologically? The answer lies in a metabolic pathway called beta-oxidation: the process by which fatty acids are systematically dismantled inside mitochondria to produce an enormous supply of ATP. Understanding how the body uses fat as fuel is not just relevant for weight management — it is central to understanding why low-intensity aerobic exercise is so important in physical therapy, how the body sustains energy during prolonged rehabilitation activities, and why cardiovascular conditioning plays such a significant role in recovery.
Fat as the Body’s Largest Energy Reserve
The body stores energy in three main forms: carbohydrates (as glycogen), proteins (as muscle mass), and fats (as triglycerides in adipose tissue). Of these, fat is by far the largest reservoir.
A lean, 70-kg adult might store:
- Approximately 400-500 grams of glycogen (providing about 1,600-2,000 kcal).
- Approximately 12-15 kg of adipose fat (providing approximately 100,000-130,000 kcal).
In other words, fat stores provide roughly 60-80 times more energy than glycogen stores. This makes fat the ideal fuel for prolonged, low-intensity physical activity — precisely the type of activity that characterizes much of early physical therapy rehabilitation: walking, cycling, swimming, aquatic therapy, and gentle functional training.
The Process of Lipolysis: Releasing Fat from Storage
Before fatty acids can be used for energy, they must be released from adipose tissue through a process called lipolysis. Adipocytes (fat cells) store triglycerides — molecules consisting of three fatty acid chains attached to a glycerol backbone.
During exercise — or during fasting or caloric deficit — hormones including epinephrine (adrenaline), norepinephrine, and glucagon activate an enzyme called hormone-sensitive lipase (HSL) inside adipocytes. HSL cleaves the fatty acid chains from glycerol, releasing free fatty acids (FFAs) into the bloodstream.
Free fatty acids travel through the blood bound to albumin (a plasma protein) and are taken up by muscle cells and other tissues that need fuel. Insulin inhibits lipolysis — which is why fat burning is maximized when insulin levels are low (during fasting or moderate exercise) and minimized after carbohydrate-rich meals.
The glycerol backbone released during lipolysis travels to the liver, where it can be converted into glucose (gluconeogenesis) — providing additional fuel during prolonged exercise or fasting.
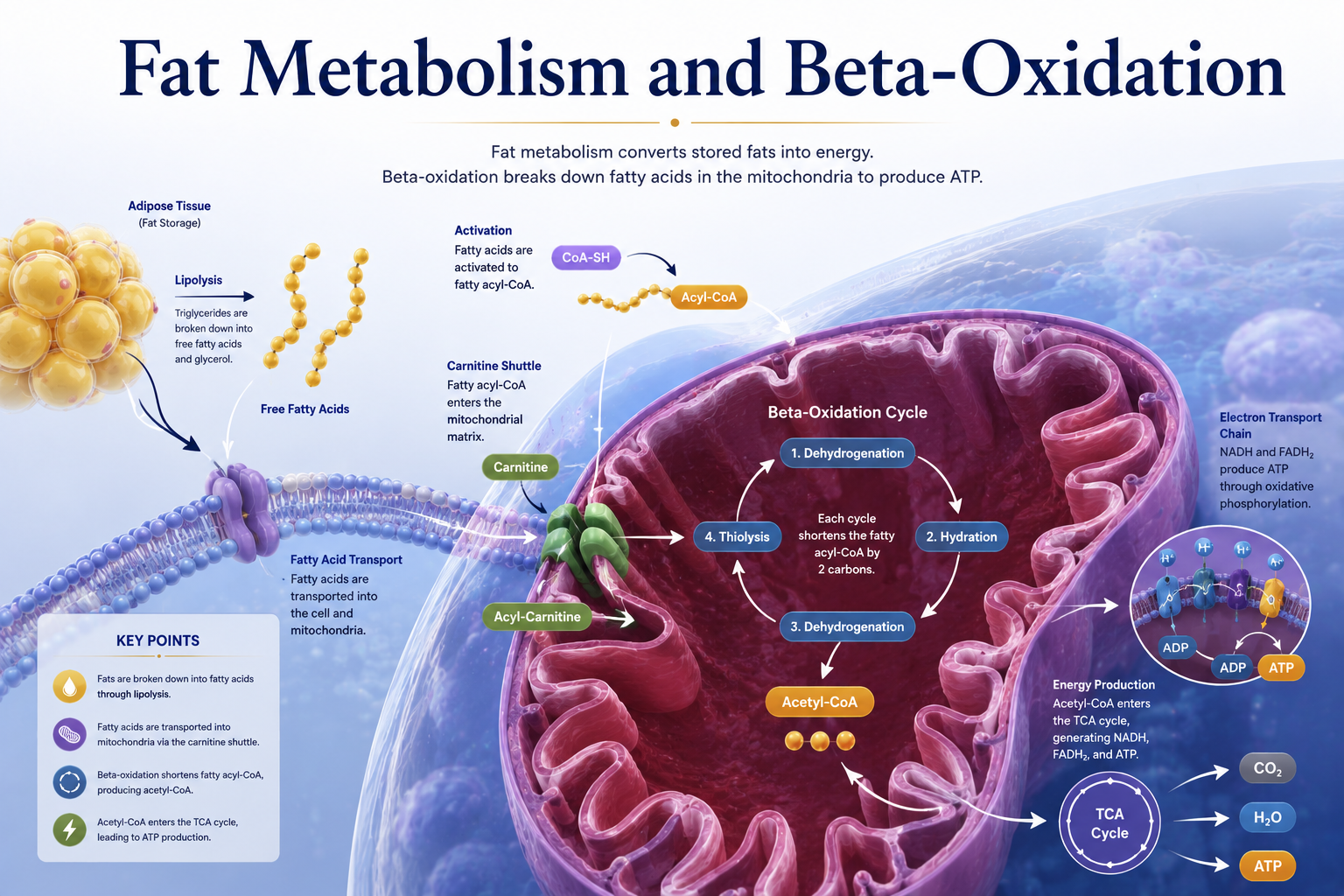
Beta-Oxidation: Dismantling Fatty Acids for Energy
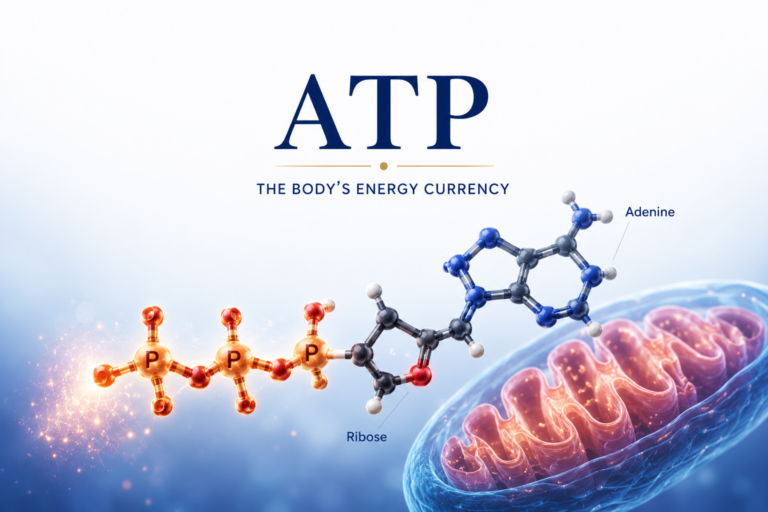
Once free fatty acids enter the cell, they are activated in the cytoplasm by combining with coenzyme A (CoA) to form acyl-CoA. This activated fatty acid is then transported into the mitochondrial matrix — the site of beta-oxidation.
Beta-oxidation is a repeating cycle of four enzymatic reactions that progressively shorten the fatty acid chain by two carbons with each cycle, releasing one acetyl-CoA molecule and producing one NADH and one FADH₂ per cycle.
The term “beta-oxidation” refers to the fact that the oxidation occurs at the beta carbon (the second carbon from the carboxyl end) of the fatty acid chain.
For a typical 16-carbon fatty acid (palmitate), beta-oxidation goes through 7 cycles, producing:
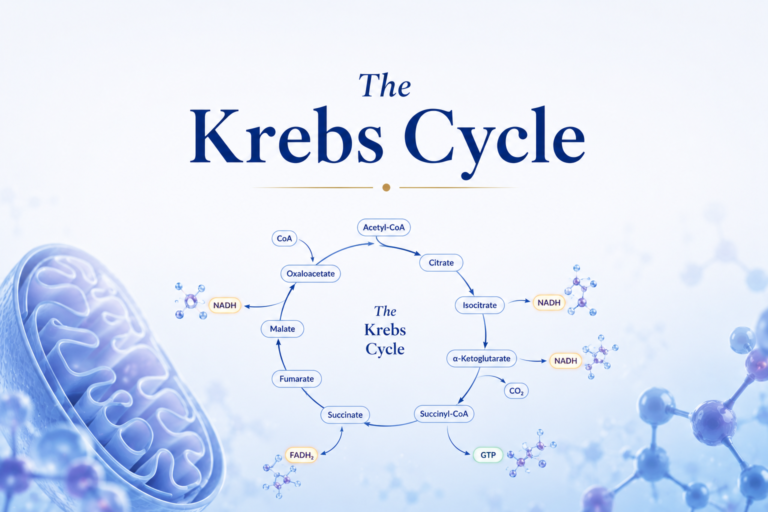
- 8 acetyl-CoA molecules (which enter the Krebs cycle)
- 7 NADH molecules
- 7 FADH₂ molecules
These products feed into the Krebs cycle and electron transport chain, ultimately generating approximately 106 ATP molecules per molecule of palmitate — compared to 30-32 ATP per glucose molecule. Gram for gram, fat provides more than twice the energy of carbohydrate (9 kcal/g vs. 4 kcal/g).
However, fat oxidation also requires more oxygen per unit of ATP produced than carbohydrate oxidation — which is why fat burning becomes less efficient (relatively speaking) as exercise intensity increases and oxygen delivery becomes limiting.
The Fat-Carbohydrate Fuel Continuum
A critical concept in exercise metabolism is that fat and carbohydrate are not used exclusively — the body uses a blend of both fuels simultaneously, with the ratio shifting based on exercise intensity and duration:
Low intensity (e.g., gentle walking, slow cycling, aquatic therapy): Fat provides the majority of energy — sometimes 60-70% or more. This is the classic “fat-burning zone” and is highly relevant to early physical therapy rehabilitation.
Moderate intensity (e.g., brisk walking, moderate cycling, functional exercises): A roughly equal mix of fat and carbohydrate. Fat oxidation is still substantial, but as intensity rises, carbohydrate contribution increases.
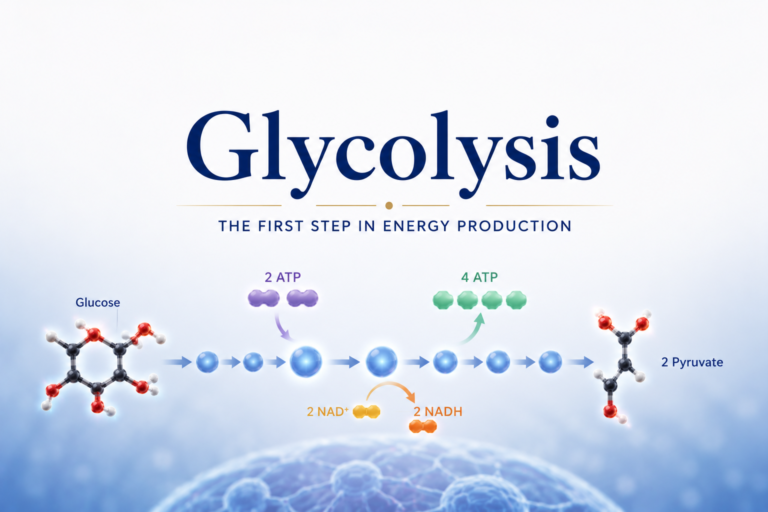
High intensity (e.g., sprint intervals, heavy resistance training): Carbohydrates dominate almost completely. At very high intensities, the rate of ATP demand exceeds what fat oxidation can supply, and the body shifts to rapid glycolysis.
Physical therapy exercise prescriptions take advantage of this continuum. For patients managing cardiovascular conditions, obesity, metabolic syndrome, or early recovery from surgery, low-to-moderate intensity aerobic exercise maximizes fat utilization while being safe and sustainable.
Aerobic Training and Fat Oxidative Capacity
One of the most significant adaptations to regular aerobic training is enhanced fat oxidation capacity. Trained individuals:
- Have more mitochondria per muscle cell (providing more sites for beta-oxidation).
- Have higher levels of fatty acid transport proteins (facilitating fatty acid uptake into muscle cells).
- Have increased activity of beta-oxidation enzymes and Krebs cycle enzymes.
- Show lower respiratory exchange ratio (RER) at any given exercise intensity (meaning more fat relative to carbohydrate is being oxidized).
These adaptations mean that aerobically trained individuals spare glycogen during exercise — relying more on fat and preserving carbohydrate for when it is most needed (high-intensity efforts). This metabolic flexibility is a hallmark of good aerobic fitness and contributes to improved exercise endurance and faster recovery.
Physical therapy programs that include regular aerobic conditioning progressively develop these fat-oxidative adaptations, making rehabilitation exercises progressively easier and more sustainable.
Fat Metabolism and Weight Management in Rehabilitation
Many physical therapy patients are managing musculoskeletal conditions that are significantly influenced by body weight — including osteoarthritis, spinal stenosis, plantar fasciitis, and stress fractures. Reducing body weight reduces the mechanical load on affected joints and structures, directly improving outcomes.
Low-intensity aerobic exercise is a cornerstone of weight management programs for several reasons:
- It is sustainable for longer durations (due to abundant fat stores and lower fatigue).
- It can be performed safely even in patients with significant joint pain (using non-weight-bearing modes like cycling or aquatic exercise).
- It improves metabolic health by increasing insulin sensitivity and fat oxidative capacity.
- It preserves muscle mass (unlike very low-calorie diets alone).
Understanding that low-intensity exercise is not “less effective” but differently effective — maximizing fat burning and cardiovascular conditioning — helps patients appreciate the value of low-intensity aerobic components of their rehabilitation programs.
Ketone Bodies: Fat Metabolism During Prolonged Fasting
When carbohydrate availability is very low (during prolonged fasting, very low-carb diets, or starvation), the liver produces ketone bodies (acetoacetate, beta-hydroxybutyrate, and acetone) from acetyl-CoA generated by beta-oxidation. These ketone bodies can be used as fuel by the brain, heart, and muscles.
Some physical therapy patients follow ketogenic diets, which significantly shift fuel metabolism toward fat and ketone body oxidation. While these diets can support weight loss and metabolic health in some contexts, they may impair high-intensity exercise performance (which depends on glycolysis) — an important consideration when planning rehabilitation programs.
Conclusion
Fat metabolism through beta-oxidation is the body’s long-term energy strategy — converting the body’s largest energy reservoir into the ATP that powers sustained physical activity. Its importance in physical therapy is enormous: low-intensity aerobic exercise, cardiovascular conditioning, weight management, and metabolic rehabilitation all depend on efficient fat utilization.
Understanding that low-intensity exercise is not “easy” in a pejorative sense, but scientifically targeted at maximizing fat oxidation and aerobic adaptation, helps physical therapy patients appreciate the full value of every component of their rehabilitation program — including the gentler sessions that build the metabolic foundation for higher-intensity work ahead.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.