The Endocrine System: Hormones That Regulate Recovery and Stress in Physical Therapy
Discover how the endocrine system regulates recovery, manages stress, and influences rehabilitation outcomes through key hormones like cortisol, growth hormone, and insulin.
Behind every muscle that contracts, every wound that heals, and every exercise adaptation that occurs during physical therapy, a complex chemical communication system is at work. The endocrine system — a network of glands and organs that produce and release hormones into the bloodstream — orchestrates many of the physiological processes that determine how quickly and how completely a patient recovers from injury or surgery.
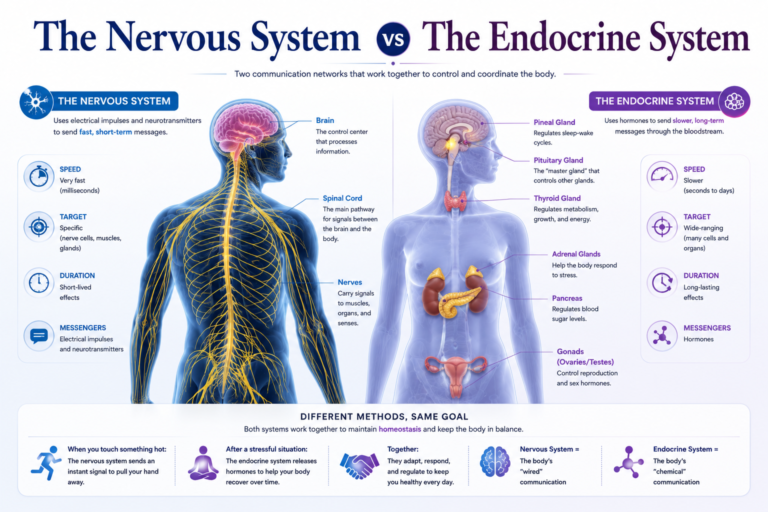
Hormones do not act like nerve signals, which produce immediate, localized effects. Instead, hormones are released into the circulation, travel throughout the body, and produce effects that may take minutes to hours to develop but can persist for days. This makes the endocrine system the body’s long-range communication network — fine-tuning metabolism, growth, inflammation, fluid balance, and psychological state in ways that profoundly influence physical therapy outcomes.
Overview of the Endocrine System
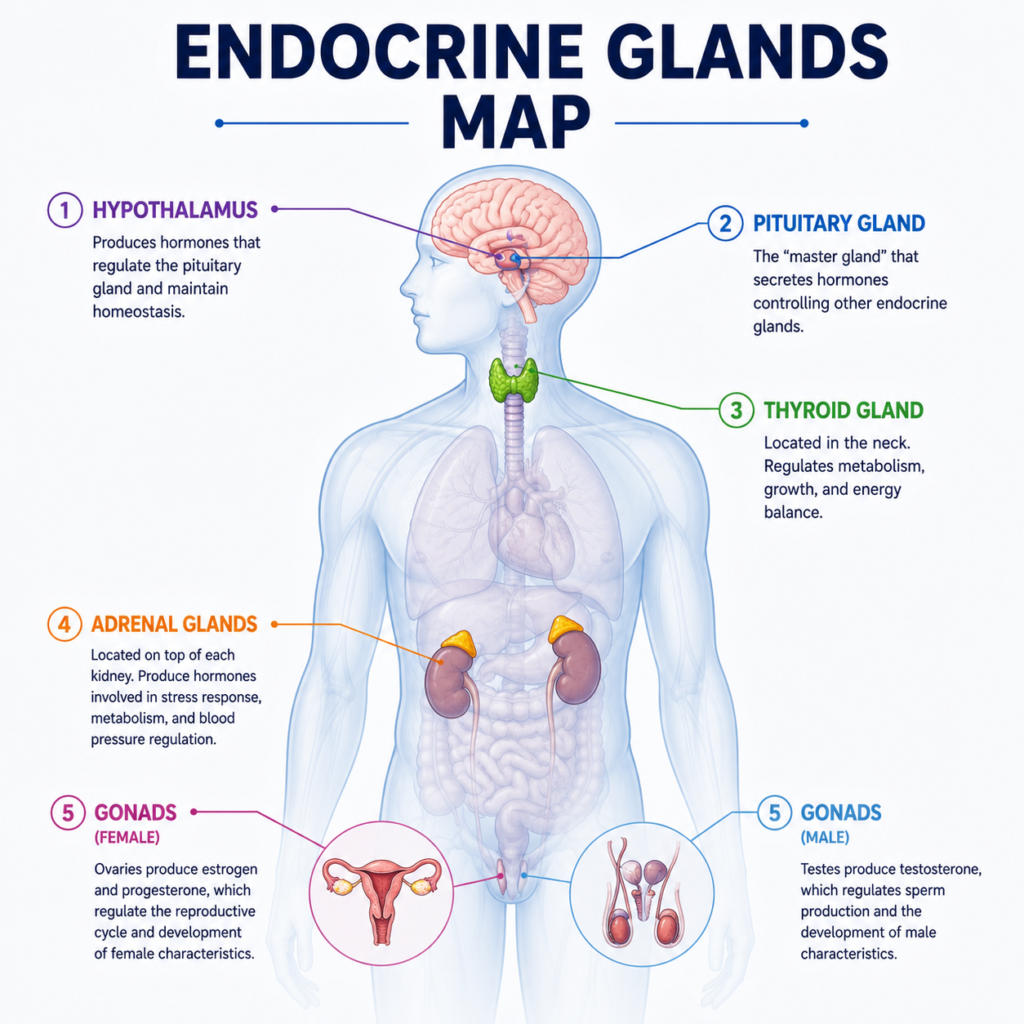
The endocrine system consists of specialized glands — including the hypothalamus, pituitary, thyroid, parathyroid, adrenal, pancreas, ovaries, and testes — as well as endocrine cells scattered throughout organs like the kidneys, heart, and gastrointestinal tract.
These glands produce hormones — chemical messengers that bind to specific receptors on target cells and alter their function. Hormone-receptor binding triggers intracellular signaling cascades that ultimately change gene expression, enzyme activity, or membrane transport, producing the hormone’s biological effect.
Hormones are classified by their chemical structure:
- Peptide/protein hormones (e.g., insulin, growth hormone, glucagon): Water-soluble, cannot cross the cell membrane, bind to surface receptors.
- Steroid hormones (e.g., cortisol, testosterone, estrogen): Lipid-soluble, can cross the cell membrane, bind to intracellular receptors that directly regulate gene expression.
- Amine hormones (e.g., epinephrine, thyroid hormones): Derived from amino acids, with properties of both groups.
Cortisol: The Double-Edged Stress Hormone
Cortisol is produced by the adrenal cortex in response to ACTH (adrenocorticotropic hormone) from the pituitary gland, which is in turn stimulated by CRH (corticotropin-releasing hormone) from the hypothalamus. Together, these form the hypothalamic-pituitary-adrenal (HPA) axis.
Cortisol is released in response to physical stress (injury, surgery, intense exercise) and psychological stress. Its biological effects include:
- Raising blood glucose (through gluconeogenesis and glycogenolysis) to ensure fuel availability during stress.
- Suppressing non-essential immune functions while redirecting resources toward immediate survival.
- Mobilizing proteins from muscle to provide amino acids for gluconeogenesis — a catabolic effect.
- Reducing inflammation by suppressing the production of inflammatory cytokines.
- Altering bone metabolism — prolonged cortisol elevation increases bone resorption and reduces bone formation.
In physical therapy, cortisol is both friend and foe. Acutely, cortisol responses to exercise and injury help mobilize resources needed for healing. But chronically elevated cortisol — from prolonged pain, psychological distress, poor sleep, or excessive training without recovery — drives muscle catabolism, impairs immune function, disrupts sleep (reducing growth hormone secretion), and can significantly slow rehabilitation.
Physical therapists increasingly recognize that psychological and social factors affect rehabilitation outcomes partly through their effects on the HPA axis and cortisol secretion. Pain neuroscience education, stress management support, and addressing fear of movement can help modulate cortisol and create a more favorable hormonal environment for recovery.
Growth Hormone: The Primary Anabolic Signal
Growth hormone (GH) is secreted by the anterior pituitary gland, primarily during deep sleep and in pulses stimulated by exercise. Its biological effects include:
- Stimulating tissue growth and repair — especially of muscle, bone, and connective tissue.
- Promoting protein synthesis — both directly and through its primary mediator, IGF-1 (insulin-like growth factor 1), which is produced mainly by the liver in response to GH.
- Increasing fat mobilization — GH promotes lipolysis, releasing fatty acids from adipose tissue for use as fuel.
- Supporting immune function — GH has immunomodulatory effects that support healing.
Growth hormone secretion is maximized during slow-wave (deep) sleep. This is one of the strongest biological reasons why adequate, high-quality sleep is essential during rehabilitation — GH secretion during sleep is the primary anabolic hormonal signal that drives overnight tissue repair.
Exercise — particularly resistance training and high-intensity aerobic exercise — also stimulates GH secretion. This is one mechanism through which therapeutic exercise accelerates recovery: it triggers GH-driven anabolic responses in muscle, tendon, and bone.
For older adults undergoing physical therapy, GH secretion declines with age (somatopause), contributing to reduced muscle mass, slower healing, and reduced exercise adaptation. This is why older rehabilitation patients may need more conservative progression and more attention to recovery optimization.
Insulin: Anabolic Orchestrator
Insulin is secreted by pancreatic beta cells in response to rising blood glucose after eating. In the context of physical therapy recovery, insulin is a key anabolic hormone:
- Facilitates glucose uptake into muscle and fat cells (lowering blood glucose).
- Promotes glycogen synthesis in muscle and liver.
- Inhibits protein breakdown in muscle — reducing catabolism.
- Supports fat storage in adipose tissue.
Exercise increases insulin sensitivity in muscle — meaning muscles become more responsive to insulin’s effects on glucose uptake, even at lower insulin levels. This is one of the most important metabolic benefits of exercise and is a key reason physical activity is prescribed for patients with type 2 diabetes and metabolic syndrome.
The post-exercise window (30-60 minutes) is a time of heightened insulin sensitivity and elevated muscle protein synthesis — making it the optimal time for protein and carbohydrate intake to support glycogen replenishment and tissue repair.
Testosterone and Estrogen: Anabolic and Bone-Protective Hormones
Sex hormones produced by the gonads (testes and ovaries) and adrenal cortex have significant effects on musculoskeletal health:
Testosterone promotes:
- Muscle protein synthesis and muscle hypertrophy (particularly in response to resistance training).
- Bone matrix deposition and mineralization.
- Red blood cell production (erythropoiesis) — relevant to oxygen-carrying capacity.
- Connective tissue resilience.
Estrogen promotes:
- Bone mineral density maintenance — estrogen inhibits osteoclast activity, protecting against bone loss. The dramatic loss of estrogen at menopause is the primary cause of postmenopausal osteoporosis.
- Ligament and tendon flexibility (estrogen increases collagen turnover).
- Anti-inflammatory effects in some tissues.
For physical therapy patients, low testosterone (hypogonadism) or estrogen deficiency (menopause) significantly affects rehabilitation. Low testosterone impairs muscle hypertrophy in response to resistance training and reduces bone density. Physical therapy programs for these patients incorporate bone-loading exercises (to maximize osteogenic stimulation) and carefully designed progressive resistance training.
Thyroid Hormones: Metabolic Rate Controllers
The thyroid gland produces thyroxine (T4) and triiodothyronine (T3), which regulate the metabolic rate of virtually every cell in the body. Thyroid hormones:
- Increase basal metabolic rate (the energy expended at rest).
- Support normal cardiac function and heart rate.
- Are essential for normal muscle contraction and relaxation speed.
- Regulate normal bone remodeling.
Hypothyroidism (underactive thyroid) — characterized by fatigue, muscle weakness, slow reflexes, and cold intolerance — significantly impairs exercise tolerance and rehabilitation progress. Physical therapists working with hypothyroid patients adjust their programs to match the patient’s reduced metabolic capacity and monitor for excessive fatigue.
Hyperthyroidism (overactive thyroid) can cause muscle weakness through a different mechanism — excessive thyroid hormone drives muscle catabolism and can impair neuromuscular coordination.
The Renin-Angiotensin-Aldosterone System: Fluid and Blood Pressure
The renin-angiotensin-aldosterone system (RAAS) regulates blood pressure and fluid balance. It is activated by low blood pressure, low blood volume, or low sodium. It ultimately stimulates the adrenal glands to release aldosterone, which causes the kidneys to retain sodium and water — increasing blood volume and pressure.
For physical therapy patients, the RAAS is relevant in two contexts:
- Post-injury edema: Aldosterone-driven sodium and water retention contributes to post-traumatic fluid accumulation.
- Cardiovascular rehabilitation: Many patients are on ACE inhibitors (which block the RAAS) for hypertension or heart failure. These medications influence blood pressure responses to exercise and require monitoring during physical therapy sessions.
Conclusion
The endocrine system is the hormonal conductor of the body’s recovery orchestra. Growth hormone drives anabolism during sleep; testosterone and estrogen maintain musculoskeletal structure; insulin coordinates nutrient storage and protein preservation; cortisol mobilizes resources during stress; and thyroid hormones keep the metabolic engine running.
Physical therapy interacts with all of these hormonal systems — stimulating anabolic hormone secretion through exercise, reducing catabolic cortisol through pain management and stress reduction, and optimizing the hormonal environment for healing through education and activity prescription. Understanding this hormonal landscape helps physical therapists design more effective, individualized rehabilitation programs and helps patients appreciate that recovery is a whole-body process, coordinated at the molecular level by the endocrine system.
References
- Hall, J.E., & Hall, M.E. (2020). Guyton and Hall Textbook of Medical Physiology (14th ed.). Elsevier.
- Costanzo, L.S. (2022). Physiology (7th ed.). Elsevier.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.
The site is written and curated by Paul Morgan, a graduate in Physiotherapy (2026), with a particular interest in cardiorespiratory and musculoskeletal physical therapy. Every article on this site is grounded in academic physiology and physical therapy coursework. Content reviewed for clinical accuracy before publishing.