Tissue Regeneration: The Science Behind How the Body Heals After Injury
Understand the three phases of tissue healing — inflammation, proliferation, and remodeling — and how physical therapy supports each stage of the regenerative process.
The human body’s capacity to heal itself is one of nature’s most remarkable achievements. A broken bone rebuilds itself to near-original strength. A torn tendon gradually restores tensile capacity. A skin wound closes and forms a scar that, though imperfect, restores the barrier function of the skin. These are not passive events — they are active, highly coordinated biological programs involving hundreds of cell types, thousands of molecular signals, and a precise temporal sequence of events.
Understanding this regenerative process is fundamental to physical therapy practice. The timing of therapeutic interventions, the type of exercises prescribed, the use of modalities like ultrasound or low-level laser, and the management of scar tissue all align with what the biology of tissue healing tells us about what the body needs at each stage of recovery.
Regeneration vs. Repair: An Important Distinction
Before exploring the stages of healing, it is worth distinguishing between two forms of tissue restoration:
True regeneration means the restoration of the original tissue type and structure. This occurs in tissues with a high cell division capacity — such as liver, skin, and bone marrow. After significant hepatic injury, the liver can regenerate to near-normal function through proliferation of remaining hepatocytes.
Repair (scar formation) means restoration of tissue continuity, but with scar tissue rather than the original tissue type. This occurs when regenerative capacity is insufficient to restore the original structure. Tendons, ligaments, and cartilage predominantly undergo repair rather than true regeneration — which is why injuries to these structures tend to leave some residual weakness or altered biomechanics, even after full clinical recovery.
Most musculoskeletal healing is a mix of both — some original cell types are restored, while scar tissue fills the gap. The goal of physical therapy is to optimize the quality of this scar tissue through mechanical loading, ensuring it is well-organized, strong, and functional.
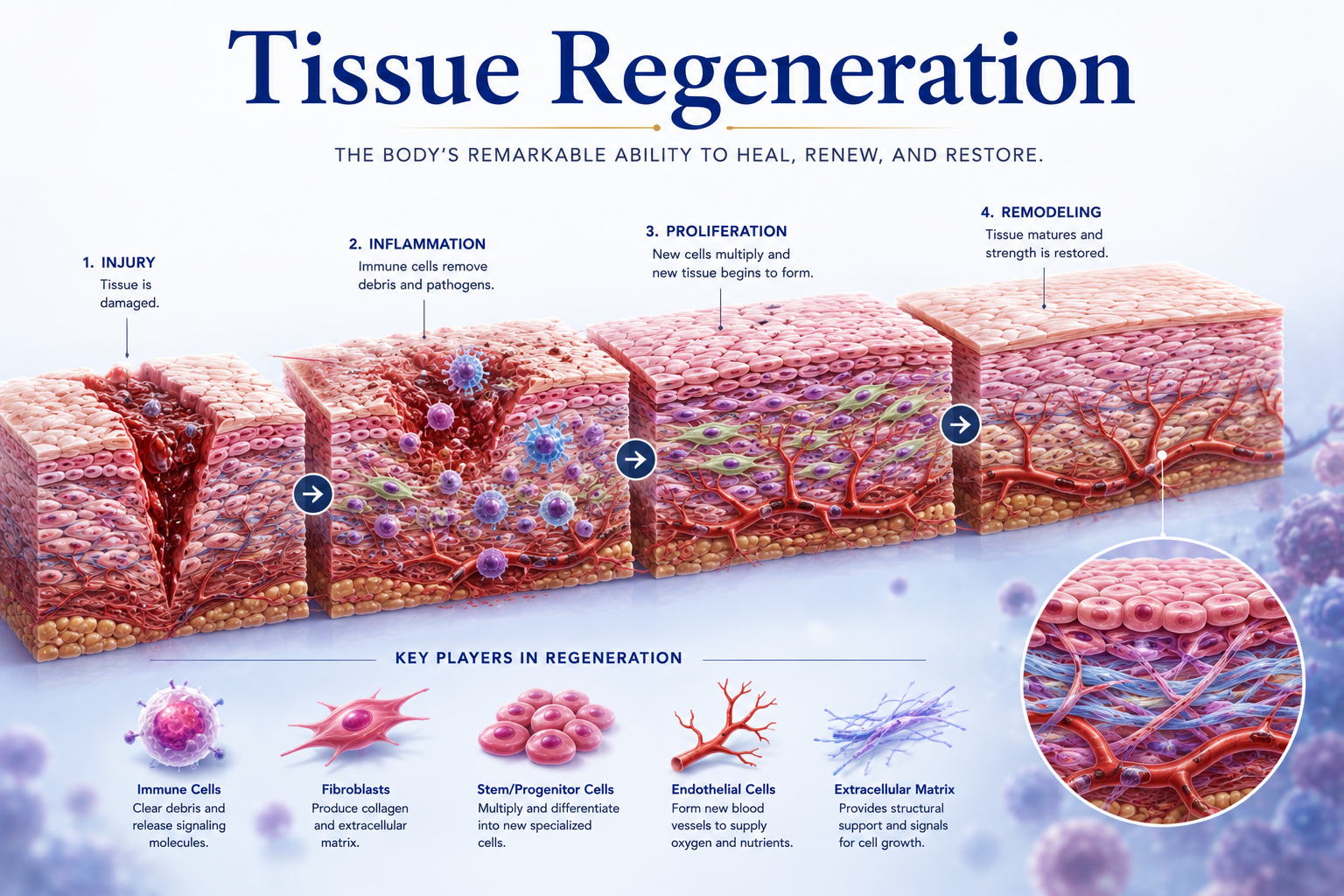
Phase 1: The Inflammatory Phase (Days 1–5)
As described in the previous articles on inflammation and the immune system, the first phase of healing is the inflammatory phase. It is activated immediately after injury and serves to:
- Control bleeding (through platelet plug formation and coagulation).
- Prevent infection (through neutrophil and macrophage activity).
- Remove damaged tissue (through phagocytosis and enzymatic degradation).
- Initiate repair (through growth factor release from platelets and macrophages).
The cardinal signs of inflammation — redness, heat, swelling, and pain — are visible manifestations of these essential biological processes.
Physical therapy during this phase is generally conservative:
- Rest from activities that aggravate the injury and risk re-injury or excessive mechanical disruption.
- Protection of the injured area from additional trauma.
- Gentle range-of-motion exercises (if tolerated and appropriate) to maintain circulation, prevent excessive stiffness, and begin providing mechanical signals to guide cell behavior.
- Edema management through elevation, compression, and lymphatic techniques.
- Pain management through ice application, gentle manual therapy, and education.
The inflammatory phase must be allowed to proceed — it is the essential foundation of healing. Therapeutic decisions during this phase focus on supporting rather than disrupting the biological process.
Phase 2: The Proliferative Phase (Days 5–21)
As the inflammatory phase resolves, the proliferative (or repair) phase begins. This is when the body actively constructs new tissue to fill the defect left by the injury. It is characterized by three overlapping processes:
Angiogenesis: New blood vessels grow into the healing tissue from surrounding vascular networks, driven by VEGF and FGF released by macrophages and platelets. These new vessels supply the oxygen and nutrients needed for the metabolically active repair process. The new tissue supplied with blood appears as a red, granular mass — called granulation tissue.
Fibroplasia: Fibroblasts — connective tissue cells — migrate into the granulation tissue and begin producing extracellular matrix, primarily Type III collagen. Type III collagen is less organized and weaker than the Type I collagen of mature connective tissue, but it is produced quickly and fills the defect. It is later replaced during remodeling. In tendon injuries, the collagen fibers are initially randomly oriented — lacking the parallel alignment that gives normal tendon its tensile strength.
Re-epithelialization: In skin wounds and mucosal injuries, epithelial cells at the wound margins begin dividing and migrating across the granulation tissue to close the defect.
Physical therapy during this phase becomes more active:
- Progressive range of motion exercises restore mobility and begin providing mechanical signals that guide collagen fiber orientation.
- Early strengthening exercises — using low load initially — begin stimulating collagen production and organization without overwhelming the fragile new tissue.
- Manual therapy and scar mobilization techniques prevent excessive fibrosis and maintain tissue mobility.
- Modalities such as therapeutic ultrasound and low-level laser therapy may support angiogenesis and fibroblast activity, though evidence varies by condition.
The mechanical environment during this phase is critically important. Fibroblasts sense the direction and magnitude of forces applied to the tissue and align their collagen fibers accordingly. Appropriate loading guides fibers along the lines of stress — improving the structural organization and mechanical properties of the repaired tissue.
Phase 3: The Remodeling Phase (Weeks to Years)
The remodeling phase is the longest phase of healing, lasting from several weeks to several years depending on the tissue type. During remodeling:
Collagen maturation: Type III collagen is gradually replaced by stronger, better-organized Type I collagen. The collagen fibers are cross-linked by the enzyme lysyl oxidase (which requires copper and requires vitamin C), increasing their tensile strength. The collagen fiber orientation improves as mechanical loading provides ongoing guidance signals.
Tissue strength recovery: The newly healed tissue gradually approaches (but rarely fully matches) the mechanical properties of the original tissue. Skin regains approximately 70–80% of pre-injury tensile strength. Tendons typically regain 80–90% of original strength within 12–16 months. Bone can restore near-original strength within 3–6 months for minor fractures.
Scar maturation: Highly vascular, cellular granulation tissue is replaced by a relatively avascular, acellular, collagen-rich scar. The scar gradually contracts, becoming more compact and pale. In some patients — particularly those with a genetic predisposition — excessive collagen production leads to hypertrophic scars or keloids.
Physical therapy during this phase focuses on:
- Progressive loading: Increasing exercise intensity and specificity to challenge the remodeling tissue progressively and stimulate optimal collagen organization.
- Sport-specific and function-specific training: Replicating the mechanical demands the tissue will face in normal use.
- Scar tissue management: Manual therapy, stretching, and massage to prevent restrictive adhesions and improve tissue mobility.
- Prevention of re-injury: The remodeling tissue remains vulnerable to re-injury for months — physical therapy ensures that progression is based on tissue tolerance, not just subjective pain levels.
Factors That Affect Healing
Multiple factors influence the pace and quality of tissue regeneration:
- Age: Healing slows with age — older tissues have fewer stem cells, reduced growth factor responsiveness, and decreased collagen synthesis rates.
- Nutrition: Protein (amino acids for collagen synthesis), vitamin C (essential for collagen maturation), vitamin D (bone healing), zinc (immune function and enzyme cofactor), and adequate calories all support healing.
- Comorbidities: Diabetes impairs healing through multiple mechanisms — reduced blood flow, impaired neutrophil function, and reduced growth factor activity. Peripheral vascular disease severely limits tissue perfusion.
- Smoking: Nicotine impairs blood vessel function, reduces tissue oxygenation, and significantly delays healing.
- Medications: Corticosteroids impair multiple phases of healing. NSAIDs affect the inflammatory and early repair phases. Anticoagulants affect hemostasis.
- Mechanical environment: The quality and quantity of mechanical loading during healing is one of the most powerful modifiable factors — and the primary domain of physical therapy.
Conclusion
Tissue regeneration is a biological masterpiece — a precisely timed, beautifully orchestrated sequence of events that rebuilds what injury has broken. The inflammatory phase clears the debris; the proliferative phase builds the scaffolding; and the remodeling phase refines the structure over months and years.
Physical therapy is the discipline that understands this timeline and provides the right mechanical, nutritional, and physiological inputs at each stage to maximize the quality of the outcome. For every patient in rehabilitation, tissue regeneration is happening right now — and every therapy session is an opportunity to make that process more efficient, more organized, and more complete.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.