White Blood Cells: The Soldiers of Immune Defense and Their Role in Physical Therapy
Learn about the different types of white blood cells, how they defend the body against injury and infection, and how physical therapy influences immune cell activity.
When an injury occurs — a torn muscle, a sprained ligament, a post-surgical wound — the body’s healing process depends on a rapid mobilization of the immune system. At the forefront of this response are the white blood cells (leukocytes): a diverse army of cells that patrol the blood and tissues, detect threats, coordinate the inflammatory response, clear damaged material, and ultimately help orchestrate tissue repair.
Understanding the different types of white blood cells, their specific roles, and how physical therapy interventions influence their activity provides a deeper appreciation of why therapeutic approaches are structured the way they are — and why supporting overall immune health is an important component of successful rehabilitation.
What Are White Blood Cells?
White blood cells (leukocytes) are the cellular components of the immune system, circulating in blood and found in lymphatic tissue. They are produced in the bone marrow from hematopoietic stem cells through a process called hematopoiesis.
In a healthy adult, the normal white blood cell count is approximately 4,500–11,000 cells per microliter of blood. This count can rise significantly during infection, injury, or intense physical exercise (a temporary phenomenon called exercise-induced leukocytosis).
White blood cells are classified into two main groups:
- Granulocytes: Cells with prominent granules in their cytoplasm — including neutrophils, eosinophils, and basophils.
- Agranulocytes: Cells without prominent granules — including monocytes/macrophages and lymphocytes.
Each type has a distinct role in immune defense, and physical therapy patients encounter the effects of all of them during the healing process.
Neutrophils: The First Responders
Neutrophils are the most abundant white blood cells, comprising 50–70% of the total white blood cell count. They are short-lived cells (surviving only hours to days) but are produced in enormous numbers (approximately 100 billion per day in an adult).
Neutrophils are the immune system’s first responders to injury and infection. Within minutes to hours of tissue damage, they are recruited from the bloodstream to the injury site by chemical signals (cytokines and chemokines) released by damaged cells and resident immune cells.
At the injury site, neutrophils perform several functions:
- Phagocytosis: They engulf and destroy bacteria and cellular debris by enclosing them in phagosomes and exposing them to digestive enzymes and reactive oxygen species.
- Degranulation: They release pre-formed granules containing proteases and antimicrobial proteins that kill pathogens and begin breaking down damaged tissue.
- Neutrophil extracellular traps (NETs): In some situations, neutrophils extrude a web of DNA and proteins that traps and kills bacteria.
In physical therapy, neutrophil activity during the first 24–48 hours after injury is essential for cleaning up the damaged site and preparing it for repair. However, excessive or prolonged neutrophil activity — as can occur with repeated injury before healing is complete — can damage surrounding healthy tissue through bystander injury from released enzymes and reactive oxygen species. This is one reason why progressive loading and adequate recovery between sessions are important.
Macrophages: The Versatile Orchestrators
Monocytes are white blood cells that circulate in the blood for 1–3 days. When they migrate into tissues, they differentiate into macrophages — one of the most versatile and powerful cells in the immune system.
Macrophages are literally “big eaters” (from the Greek makros + phagein). They phagocytose larger particles than neutrophils can — including apoptotic neutrophils, damaged cellular debris, and even entire dead cells. But their role goes far beyond eating.
In tissue healing, macrophages exist on a spectrum of functional states, classically described as M1 and M2 phenotypes:
M1 macrophages (pro-inflammatory/classically activated) dominate in the early phase of healing. They:
- Produce pro-inflammatory cytokines (TNF-α, IL-1β, IL-6) that amplify the inflammatory response.
- Kill bacteria and damaged cells.
- Recruit additional immune cells to the site.
M2 macrophages (anti-inflammatory/alternatively activated) become dominant as healing progresses. They:
- Produce anti-inflammatory cytokines (IL-10, TGF-β) that resolve inflammation.
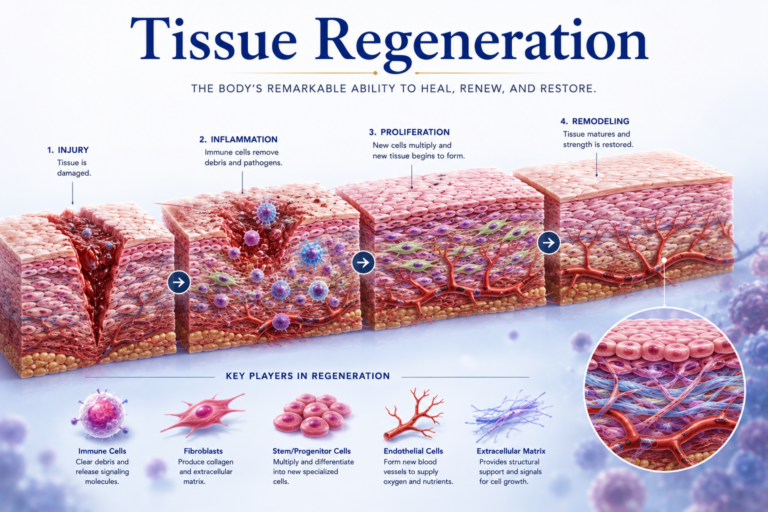
- Release growth factors (VEGF, PDGF, TGF-β) that stimulate fibroblast activity, new blood vessel formation, and collagen production.
- Promote the transition from inflammation to tissue repair.
The timely transition from M1 to M2 macrophage dominance is essential for normal healing. Conditions that impair this transition — including chronic stress, poor nutrition, and persistent infection — lead to chronic non-resolving inflammation and impaired tissue repair. Physical therapy interventions may support this transition through exercise-mediated anti-inflammatory signaling and the mechanical stimuli that guide macrophage behavior.
Lymphocytes: Specific, Memory-Based Defense
Lymphocytes are the cells of the adaptive immune system, comprising approximately 20–35% of white blood cells. They come in two main types:
B lymphocytes (B cells) produce antibodies — highly specific proteins that bind to particular antigens (foreign molecules) and mark pathogens for destruction by other immune cells. Antibodies can also directly neutralize toxins and prevent viral particles from entering cells.
T lymphocytes (T cells) include:
- Cytotoxic T cells (CD8⁺): Directly kill virus-infected cells and cancer cells.
- Helper T cells (CD4⁺): Coordinate the immune response by producing cytokines that activate B cells, cytotoxic T cells, and macrophages.
- Regulatory T cells (Tregs): Suppress excessive immune activity, preventing autoimmune responses.
In the context of physical therapy and musculoskeletal healing, lymphocytes are primarily relevant in:
- Infections: Adaptive immunity is essential for clearing bacterial or viral infections that can complicate post-surgical or post-traumatic healing.
- Autoimmune conditions: Dysregulated T cell activity drives autoimmune destruction of joints (as in rheumatoid arthritis) — physical therapy management is adapted to the autoimmune inflammatory environment.
- Chronic tendinopathy: Research has identified T lymphocyte infiltration in chronically diseased tendons, suggesting an adaptive immune component in this condition.
Eosinophils and Basophils: Supporting Roles
Eosinophils and basophils are less numerous granulocytes (typically less than 5% of white blood cells combined), with specialized roles:
Eosinophils are involved primarily in allergic reactions and defense against parasitic infections. In physical therapy practice, they are most relevant in patients with asthma or allergic conditions, where eosinophil-driven airway inflammation affects exercise tolerance and respiratory function.
Basophils and their tissue-resident cousins, mast cells, release histamine and other inflammatory mediators in response to allergic stimuli. Mast cells in connective tissue play a role in the initial inflammatory response to injury, contributing to the immediate vasodilation and permeability changes seen in the first minutes after trauma.
Exercise and White Blood Cell Activity
Exercise has well-documented effects on white blood cells:
Acute effects: During moderate to vigorous exercise, the number of circulating leukocytes increases significantly — particularly neutrophils and natural killer cells. This exercise-induced leukocytosis is driven by catecholamine release (epinephrine), which causes immune cells to be mobilized from storage sites in the spleen and blood vessel walls. For 1–3 hours after intense exercise, there may be a temporary redistribution and functional impairment of some immune cells.
Chronic effects of regular exercise: Long-term moderate exercise training improves immune surveillance, enhances macrophage function, increases natural killer cell activity, and reduces the baseline level of pro-inflammatory cytokines (CRP, IL-6, TNF-α). These systemic anti-inflammatory effects contribute to the overall health benefits of physical activity.
For physical therapy rehabilitation, this means:
- Regular moderate exercise enhances immune function and supports healing.
- Excessive exercise intensity or volume without adequate recovery can temporarily impair immunity, increasing infection risk and potentially impairing tissue repair.
- The progressive exercise prescription used in physical therapy is designed to maximize beneficial immune adaptations while avoiding immunosuppressive overload.
Nutrition and White Blood Cell Function
White blood cells depend on adequate nutrition for optimal function:
- Zinc is essential for T cell development and function. Zinc deficiency is associated with impaired immune responses.
- Vitamin C supports neutrophil function, antioxidant defense, and collagen synthesis.
- Vitamin D has significant immunomodulatory effects — deficiency is associated with impaired innate immunity and increased susceptibility to infection.
- Protein provides the amino acids needed for antibody production and white blood cell synthesis.
Physical therapy patients recovering from injury or surgery often have increased nutritional demands. Supporting adequate intake of these immune-supporting nutrients is an important, if often overlooked, component of comprehensive rehabilitation.
Conclusion
White blood cells are the cellular agents of immunity and healing — neutrophils clearing debris, macrophages orchestrating repair, lymphocytes providing specific defense and memory. In physical therapy, their activity underlies every phase of the healing process, from the immediate inflammatory response to the gradual remodeling of repaired tissue.
Physical therapy supports white blood cell function through appropriate exercise (which enhances immune surveillance and promotes the anti-inflammatory M2 macrophage phenotype), timing of interventions (respecting the natural phases of immune activity during healing), and education about supporting nutrition and overall health. Understanding these cells deepens the appreciation for what is truly happening inside the body during rehabilitation — and why thoughtful, evidence-based physical therapy makes such a meaningful difference.
Disclaimer: This article is for educational purposes only and does not constitute medical advice. Always consult a qualified healthcare professional for personal health concerns.